



A Review of the Current Trends in Chronic Wound and Scar Management
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Wounds or HMP Global, their employees, and affiliates.
Abstract
Background: Aberrant tissue repair can result in the formation of chronic wounds and pathological scarring, which can severely impact a patient’s quality of life. Due to their complexity, treatment of these conditions remains challenging. Purpose: This review article provides a brief overview of the various treatments with regards to application, possible mechanism(s) of action, new developments, and areas requiring further research. Methods: A literature review on the different therapies/products currently used for chronic wounds and pathological scars was conducted. Several databases—including PubMed, ScienceDirect, Web of Science, and Google Scholar—were searched to find relevant articles on this topic. Results: Numerous products and treatment options, including several promising new technologies, are currently available. These therapies/products aim to accelerate wound healing, reduce scarring, and ultimately reach the goal of scarless tissue regeneration. Conclusion: Currently, no gold standard therapy exists for chronic wounds and pathological scars. Existing treatments demonstrate varying levels of efficacy, and further research is required regarding their safety and molecular mechanism(s) of action.
Introduction
Wound healing is a complex process that is necessary to restore the skin’s function following injury. Normal tissue repair of acute wounds occurs in 4 distinct but overlapping phases known as hemostasis, inflammation, proliferation, and remodeling.1 A disruption or delay in one of these phases results in non-healing, chronic wounds. Chronic wounds have a significant impact on the economy, health care systems, and the patient’s quality of life.1 The rising incidence of chronic conditions associated with impaired wound healing (eg, diabetes) also contributes to the problem.2
Scar tissue formation is a normal part of the tissue repair process. Depending on the depth of the wound, scarring can range from minimal (ie, superficial wounds) to severe pathological scarring.3 Excessive scarring can be debilitating, causing physical and psychological distress to the patient.3
Treatment of chronic wounds and pathological scars remains challenging due to their complexity. Various treatment options are available to promote wound healing, improve scar aesthetics, and prevent scar formation. Although scarless wound healing is the preferred outcome, none of the available treatments are capable of achieving complete skin regeneration.3 The current review article provides a brief overview of the different treatment options with regards to application, possible mechanism(s) of action, therapies/products available on the market, new developments, and areas that require further research.
Methods
Databases (including PubMed, Science Direct, Web of Science, and Google Scholar) were used to search for appropriate publications. Different combinations of the following keywords were used: chronic wounds, non-healing wounds, tissue repair, hypertrophic scars, keloids, pathological scarring, treatments. Only English-language full-text articles considered to be relevant and published between 2018 and 2023 were reviewed. The compiled reference list was used to identify any further papers of interest.
Discussion
Normal tissue repair: the 4 phases of wound healing
The first phase of wound healing—hemostasis—is triggered at the onset of injury, resulting in localized constriction of the blood vessels (vasoconstriction) and blood clot formation to prevent blood loss and serve as a provisional matrix for cell migration.1 Molecular signals such as damage-associated and pathogen-associated molecular patterns stimulate the release of pro-inflammatory mediators via Toll-like receptor signaling.4-7 This triggers the infiltration of various immune cells at the site of injury, which signals the start of the inflammatory phase of wound healing.1 Immune cells such as neutrophils and inflammatory or M1-phenotype macrophages are responsible for removal of cellular debris and extracellular pathogens.1 Multiple factors facilitate the transition from the inflammatory phase to the proliferative phase, in particular the transition of M1 macrophages to anti-inflammatory or M2-phenotype macrophages.8 M2-phenotype macrophages produce various growth factors, chemokines, and matrix metalloproteinases (MMPs) to stimulate proliferation of several different cell types and facilitate their migration to the wound site.8 Fibroblasts are responsible for replacing the provisional matrix with granulation tissue—which consists of various extracellular matrix (ECM) components such as procollagen, elastin, and proteoglycans—as well as newly formed blood vessels.8 Keratinocytes at the wound edges proliferate and migrate across the newly formed matrix to close the wound and restore the skin’s barrier function.8 Wound closure signals the start of the remodeling or scar maturation phase. During this phase, the granulation tissue matures into normal scar tissue, which involves a reduction in wound size, a decline in angiogenesis (blood vessel formation), and reorganization of the ECM.1 Myofibroblasts, the main cell type responsible for remodeling, differentiate from fibroblasts in response to cytokines (eg, transforming growth factor beta, TGF-β) and mechanical stress within the wound.1 Myofibroblasts produce various MMPs and type I collagen.8 The MMPs degrade the disorganized type III collagen fibers produced during the proliferative phase, which are then replaced with stronger type I collagen fibers.8 Although type I collagen greatly increases the strength and flexibility of the new tissue, the scar only recovers approximately 80% of the tensile strength it had prior to injury.8 Myofibroblasts also express α-smooth muscle actin which aids in contraction of the scar tissue, thus reducing its surface area.1
Inflammation, chronic wounds, and pathological scarring
Chronic wounds
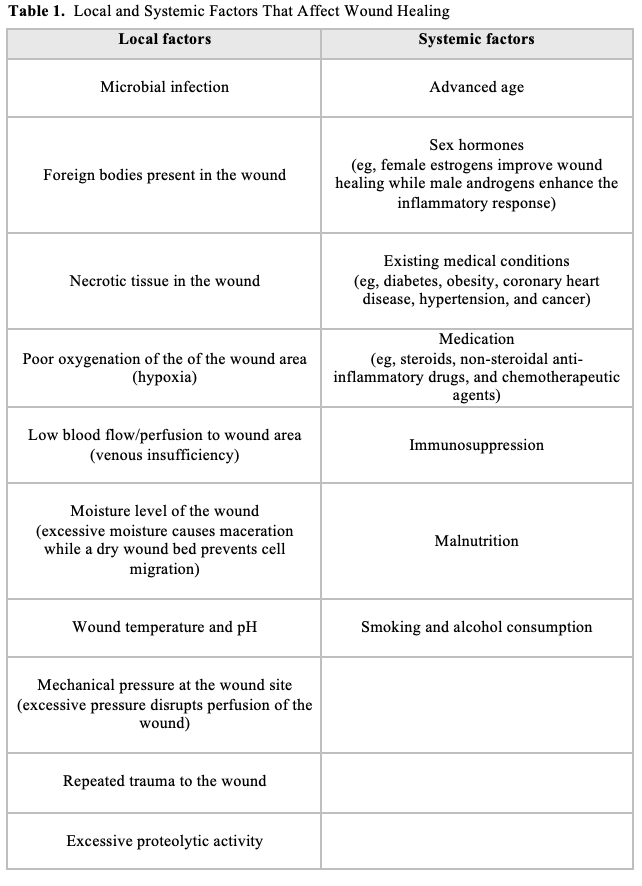
Chronic wounds (eg, diabetic ulcers, pressure ulcers and vascular ulcers) are defined as acute wounds that do not progress through the normal tissue repair process in the expected time frame.9 Various local and systemic factors can significantly delay tissue repair (Table 1) including medical conditions (eg, diabetes), a weakened immune system, certain medications (eg, steroids), age-related complications, malnutrition, and infection.10
Regardless of wound etiology, all chronic wounds are characterized by a prolonged and elevated inflammatory phase due to dysregulation of the immune response. In particular, aberrant M1 macrophage activity delays the transition from inflammation to proliferation.1 Various signals contribute to aberrant M1 macrophage activity, including high levels of iron (characteristic of chronic venous ulcers), hyperglycemia, and impaired peroxisome proliferator-activated receptor gamma activity (characteristic of diabetic ulcers).11 The M1 macrophages have limited capability for removal of neutrophils (efferocytosis), resulting in extended neutrophil activity and excessive protease (eg, MMPs and serine proteases) and reactive oxygen species (ROS) production.12 Furthermore, M1 macrophages also produce various MMPs which contribute to the pro-inflammatory environment.12
MMPs play a vital role in all stages of the wound healing process.13 These enzymes are responsible for degradation of ECM components and basement membranes to allow wound debridement, angiogenesis, cell migration, and ECM remodelling.13 MMPs can also modulate the activity of numerous cytokines, chemokines, growth factors, cell receptors, and proteases that regulate cellular processes such as inflammation and cell death (apoptosis).13 During normal tissue repair, the activity of these enzymes is tightly controlled via several mechanisms, including endogenous tissue inhibitors of metalloproteinases (TIMPs).14 In chronic wounds, MMP activity is upregulated while TIMP levels are aberrantly low.14 This disturbance in the MMP/TIMP equilibrium is responsible for increased ECM turnover and degradation of cytokines, growth factors, and protease inhibitors, which impairs wound healing.14
Cellular senescence is another potential factor that contributes to the pro-inflammatory wound environment.15-17 Studies have demonstrated that senescent cells, in particular macrophages and fibroblasts, accumulate within diabetic ulcers and acute wounds of aged mice.16 These cells cease to proliferate and display a pro-inflammatory senescence-associated phenotype resulting in excessive secretion of pro-inflammatory cytokines, growth factors, and proteases.16,17
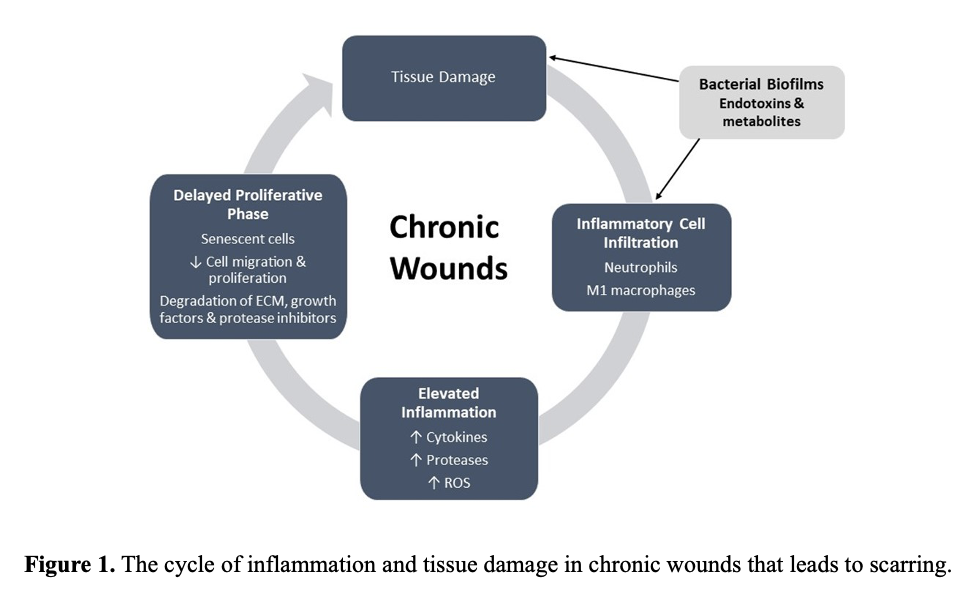
Bacterial biofilms, present in approximately 60% to 80% of chronic wounds, also contribute to wound chronicity.18 Pathogens secrete various proteases responsible for ECM degradation or activation of host MMPs.13 In addition, bacterial metabolites and endotoxins released in the wound environment cause a continuous influx of immune cells and the subsequent release of pro-inflammatory mediators.8 Overall, the pro-inflammatory environment has a wide range of consequences, including reduced angiogenesis, degradation of factors essential for healing (eg, growth factors, ECM components, and protease inhibitors), and senescent cells (eg, endothelial cells, fibroblasts, and keratinocytes) that do not proliferate and migrate to the site of injury.19 All of the above-mentioned consequences further amplify inflammation and tissue damage, resulting in a continuous, self-sustaining cycle (Figure 1).19 A more detailed discussion regarding the immune response in acute and chronic wounds was published recently.7
Scarring
Pathological scarring primarily occurs in the form of hypertrophic or keloid scars. Both scar types are characterized by excessive fibrotic tissue and share many other similarities that can complicate a differential diagnosis.20 As these scars require different therapeutic approaches, extensive research has been done to identify clinical, histological, and cellular differences between keloid and hypertrophic scars (Table 2).20
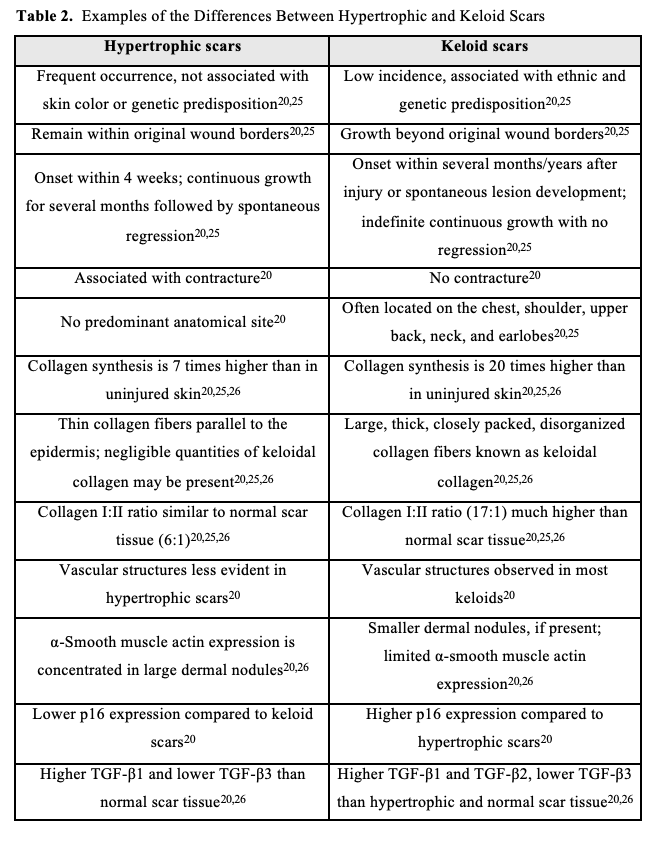
Hypertrophic scars are defined as thick, elevated scars that are confined to the original wound margins.21 Although similar in appearance, keloid scars extend beyond the wound margins into the healthy surrounding skin.21 Hypertrophic scarring is more common than keloids, appears within a short period after wound closure, and will generally mature and regress to some extent over time.20 Hypertrophic scars are also associated with contractures that can significantly reduce joint mobility, a characteristic that is not seen in keloid scars. Keloids can appear directly after wound closure, several months or years after injury, or as spontaneous lesions.20 This scar type demonstrates continuous growth without regression and has a higher rate of recurrence, thus requiring a more aggressive therapeutic approach. Some families and ethnic groups (especially those with darker skin types) demonstrate a genetic predisposition to keloid scar development.22 Keloid scars develop at certain preferential anatomical sites (eg, the chest, shoulders, neck, back, and earlobes) which are frequently subjected to mechanical tension and stretching.20,23
The presence of keloidal collagen (ie, thick collagen fibers) in keloid scars versus the presence of α-smooth muscle actin concentrated in dermal nodules in hypertrophic scars have been proposed as distinguishing characteristics.20 However, dermal nodules and α-smooth muscle actin have also been observed in some keloids and were even absent from some hypertrophic scars.20 Furthermore, keloidal collagen is not present in all keloids, and a few cases have been reported where keloidal collagen was found in hypertrophic scars.20 A study by Limandjaja et al reported that even though keloid and hypertrophic scars demonstrated similar characteristics (ie, phenotypes), gradient differences in keloidal collagen, α-smooth muscle actin, and p16 (tumor suppressor protein associated with cellular senescence) existed between the two.24 A 2021 review by Limandjaja et al offers a more detailed discussion on the similarities and differences between keloid and hypertrophic scars.20
The pathogenesis of hypertrophic and keloid scars is still poorly understood; however, continuous inflammation (particularly in the reticular dermis), delayed wound healing (ie, chronic wounds), and aberrant tissue remodeling all have a significant impact on scar formation.25,27,28 The role of inflammation in scarring has been demonstrated in several instances. Early fetal wound healing (up to ± 22 weeks’ gestation) is characterized by an absent or weak inflammatory response resulting in scarless healing or skin regeneration.25 However, as the fetal skin matures the inflammatory response becomes stronger, causing fibrotic wound healing to occur.25 Studies have demonstrated that inducing inflammation during early gestation resulted in fibrotic healing.29,30 Compared to adult dermal wounds, fetal wounds have significantly lower levels of immune cells (eg, macrophages, neutrophils, and mast cells) and pro-inflammatory mediators (eg, interleukin[IL]-6 and IL-8), while anti-inflammatory cytokine levels (eg, IL-10) are upregulated.25,31 Similarly, adult oral mucosal wounds heal rapidly with minimal inflammation and scarring.25 Immune cell infiltration in oral wounds is also significantly lower than in dermal wounds and several pro-inflammatory cytokines are absent (eg, IL-23 and IL-24) or only briefly produced (eg, IL-6 and IL-8).25 The effect of inflammation on wound healing and scarring has also been observed in animal models such as PU.1 null mice. Although these mice are genetically incapable of an inflammatory response, skin wound healing occurs rapidly without scar tissue formation.32
Various inflammatory cell types, mediators, and signaling pathways are significantly upregulated in aberrant scars, especially in keloids that display a strong inflammatory response.20,33 Immune cells such as the M2-phenotype macrophages, mast cells, and T-lymphocytes are elevated to varying degrees in both scar types.20,33 Growth factors produced by these cells, such as TGF-β, are one of the primary causes of fibrosis.28 TGF-β stimulates fibroblast proliferation, migration, and differentiation into myofibroblasts.28 Keloid and hypertrophic scar fibroblasts/myofibroblasts also have more growth factor receptors, resulting in an abnormal response to TGF-β stimulation which produces excess collagen.21,34 In vivo studies have also demonstrated the pro-fibrotic effects of several pro-inflammatory mediators produced by immune cells (eg, CXCL12, monocyte chemoattractant protein-1, and IL-17).35,36 The nuclear factor-kappa B (NF-κB) pathway, which regulates inflammatory gene expression, is upregulated in keloid fibroblasts.37,38 Inhibition of this pathway significantly reduced fibroblast proliferation and type I collagen deposition. Both keloid and hypertrophic scar fibroblasts demonstrated upregulated signal transducer and activator of transcription signaling, which regulates inflammation, the proliferation and migration of fibroblasts, and collagen synthesis.39,40 Mechanical tension following injury or surgery stimulates focal adhesion kinase (FAK) signaling, which has been implicated in fibrosis. FAK signaling was found to be upregulated in both keloid and hypertrophic scars, and it accelerates fibrosis by promoting inflammation.41,42
Fibrosis can also occur due to an imbalance between collagen deposition and degradation.34 This occurs primarily due to dysregulation of MMPs and their inhibitors (TIMPs).26,34 Studies have reported decreased MMP activity (or slightly increased activity of certain MMPs), and increased or unchanged TIMP activity in different scar tissues.20,26 Overall, scar tissue displays a lower MMP to TIMP ratio, resulting in collagen accumulation.34 Proteoglycans in the ECM, such as decorin, also play an important role in tissue repair and remodeling.43 Decorin is involved in collagen fiber organization, suppression of TGF-β activity, and stimulation of fibroblast apoptosis.43 Compared to healthy tissue, decorin levels in scar tissue were found to be much lower, contributing to disorganized collagen fibers and continuous TGF-β activity.43 The role of other proteoglycans in wound repair and scarring are discussed in detail in recent reviews.44,45
Current treatment strategies for chronic wounds
Chronic wound treatment is a complex process and requires a holistic approach. When considering a treatment protocol, patient assessment is equally as important as evaluation of the wound itself.9,46 Factors such as medical history, lifestyle, underlying comorbidities, chronic medications used, the patient’s ability to adhere to treatment protocols, and the patient’s psychological well-being can all affect treatment outcome.9 The wound itself requires continuous evaluation to determine treatment efficacy. The TIME principle has been widely applied to identify and address factors that delay tissue repair.46,47 The TIME principle refers to:
- Tissue (T) – Assessment of non-viable tissue (eg, necrotic, eschar, and slough) present in the wound bed that can delay tissue repair. Non-viable tissue should be removed by means of surgical, mechanical, enzymatic, or biological debridement.
- Infection/Inflammation (I) – Assessment and management of microbial levels in the wound bed, as well as abnormal inflammation that is not related to infection.
- Moisture (M) – Assessment and management of wound exudate. Insufficient exudate (ie, dry wounds) slows down cell migration and wound healing, while excessive exudate increases the risk of infection and causes maceration of the surrounding tissue.
- Edge of wound (E) – Continuous assessment of the wound edges and surrounding skin to ensure wound progression and closure. Non-advancing wound edges indicate delayed healing and requires reassessment of the current treatment protocol.
Overall, current wound treatment strategies aim to prevent or reduce infection, create a favorable wound environment to expedite the tissue repair process, reduce the discomfort and pain of the patient, and decrease the risk of scarring.2 Current strategies include biofilm-based wound management and protease modulation with various types of wound dressings, topical treatments, and negative pressure wound therapy (NPWT).
Biofilm-based wound management and protease modulation
As discussed in the previous section, the presence of bacterial biofilms and high levels of proteases in chronic wounds contributes to wound chronicity and delayed healing. Biofilm eradication is extremely difficult due to its high tolerance and resistance to antimicrobial agents and the host’s immune response.48 Thus, conventional antibiotic treatment alone is inadequate. Surgical/sharp and mechanical debridement are critical treatment strategies to manage biofilms; however, these methods do not remove the entire biofilm and regrowth occurs rapidly.49 Current biofilm-based wound care is a holistic approach consisting of repetitive debridement to disrupt biofilms and increase antimicrobial susceptibility, followed by wound cleansing with topical antimicrobials to prevent biofilm reformation (Table 3).49 In cases where clinical signs of infection are present, this approach can be augmented with systemic antibiotics. The frequency of this approach is patient-specific and can be reduced once the wound improves, or reassessed if wound healing fails.
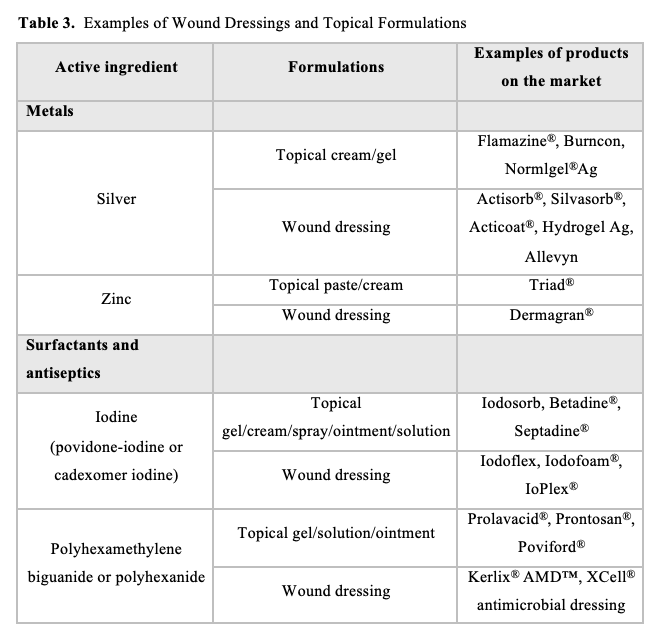
Surfactants, primarily from the betaine and poloxamer classes, play an important role in biofilm management and reducing inflammation via protease modulation, without adversely affecting cellular activity for wound healing.50 A variety of surfactant-based topical formulations (eg, gels and creams), wound dressings, and wound irrigation solutions have demonstrated efficacy in chronic wound healing.50,51 Surfactants aid in the debridement of the wound bed and may exhibit bacteriostatic (preventing bacterial growth) and/or bactericidal (killing of bacteria) activity by targeting the bacterial cell membrane; they also have antibiofilm properties.50,52 Surfactants are often used in combination with antibiotics and other antimicrobial agents such as polyhexamethylene biguanide or polyhexanide, chlorhexidine, iodine (povidone- and cadexomer-iodine), and silver nanoparticles.50,51,53 In wound dressings, the surfactant enhances the stability and activity of the antimicrobial agent and allows gradual release of antibiotics to prevent keratinocyte and fibroblast toxicity.51 The surfactant also disrupts biofilm matrix structures, which improves the penetration and antibiofilm effects of the antimicrobial agent.50,52
Protease modulation is another important treatment strategy to reduce protease activity responsible for the persistent inflammation in chronic wounds. Some surfactants (eg, poloxamer-based) and antimicrobials (eg, silver) used for wound cleansing have also demonstrated anti-inflammatory and MMP-inhibitory activity.50,54,55 The antibiotic doxycycline is a known competitive MMP inhibitor and has demonstrated improved healing outcomes in patients with diabetic foot ulcers and chronic venous ulcers.56,57 Various protease modulating wound dressings have also been developed. These dressings absorb inflammatory wound exudate, bind proteases by acting as a substrate, and/or inhibit protease activity.58
NPWT is another technique used for both wound bed debridement and protease modulation. It involves the application of subatmospheric pressure (between -80 mm Hg and -150 mm Hg) to the wound, which reduces inflammatory wound exudate (ie, protease levels) while increasing debridement, blood flow (vascular perfusion), and tissue granulation.59,60 Clinical trials have demonstrated a significant reduction in wound size and healing time with NPWT compared to standard wound care.61 NPWT with instillation (NPWTi) has the added advantage of allowing a topical solution (eg, antimicrobial) to dwell in the wound at set intervals to facilitate regular wound cleansing. In vitro and in vivo studies have demonstrated a significant reduction in bacterial biofilm load when NPWTi of various antimicrobial solutions is used, compared to NPWT alone.62,63
Skin substitutes
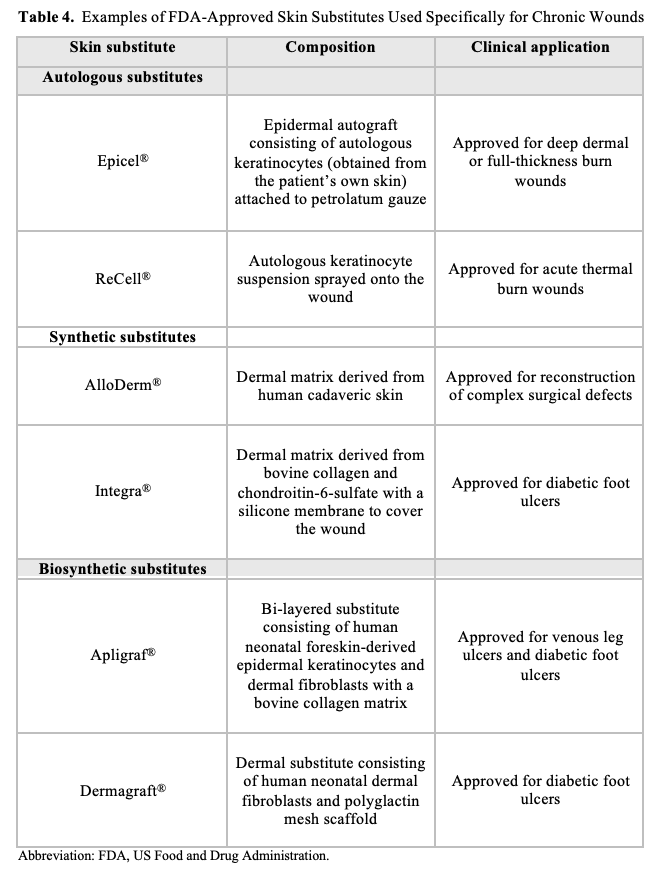
Burn wounds, chronic wounds, and other traumatic injuries often require skin substitutes to aid in wound closure, promote the repair process, and restore skin function. Skin substitutes are classified based on composition (eg, biological, synthetic, or biosynthetic materials), skin layer components (eg, epidermis, dermis, or composite), and durability (eg, temporary or permanent).64 Biological skin substitutes include allografts (ie, skin transplanted from a human donor) and xenografts (ie, dermal substitutes harvested from animal origin, generally from porcine).64 Full-thickness skin grafts consist of the epidermal and dermal skin layers, while partial- or split-thickness skin grafts consist of the epidermis and only part of the dermis.65 Skin grafts have several disadvantages, including donor rejection, risk of disease transmission from unrelated donors, insufficient harvest sites for autografts (eg, severe burn wounds over large parts of the body), and graft failure due to wound bed infection.66
To overcome these disadvantages several synthetic and bio-engineered skin substitutes have been developed (Table 4).64,66 Synthetic or acellular substitutes consist of either natural or synthetic polymers and provide a scaffold for neodermal formation and temporary closure of the wound surface.66 Biosynthetic substitutes consist of skin cells (from the patient or a donor) embedded into an acellular matrix (support structure).66
Current tissue engineering methods used to manufacture skin substitutes (eg, electrospinning, casting, freeze-drying, etc.) are unable to accurately reproduce the skin’s complex structure.66 Three-dimensional bioprinting is a novel method that has been used successfully to produce complex skin substitutes and dermal scaffolds with precision.66 Bioprinted scaffolds, with and without additives (eg, antibiotics, growth factors, drugs, etc.), and skin substitutes have demonstrated efficacy in various aspects of wound healing in vivo.66
Current treatment strategies for pathological scars
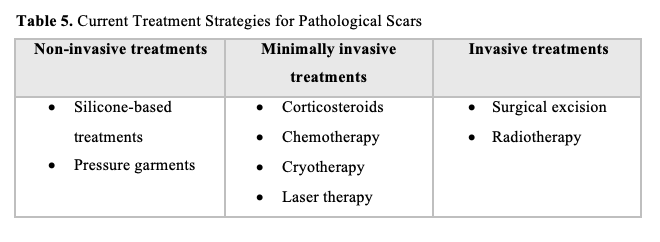
Treatment of pathological scars is challenging due to their high rate of recurrence, especially keloid scars, as well as limited knowledge regarding the molecular mechanisms responsible for their development.67 Various treatment strategies exist to prevent and reduce pathological scarring, however, there is currently no universal standard treatment regimen as the efficacy of these strategies differ significantly between patients.67 Current anti-scarring strategies mainly target and aim to reduce chronic inflammation (anti-inflammatory treatments) during the early stage of wound healing, as well as excessive collagen synthesis (anti-fibrotic treatments) during tissue remodelling.33 These strategies range from non- or minimally invasive therapies to various invasive surgical options (Table 5).
Non-invasive treatments
Silicone-based treatments. For many decades, silicone-based treatments have been used to prevent hypertrophic and keloid scar formation and reduce existing scars.68 A wide range of topical silicone-based products are currently available including silicone gels, creams, sheets/patches, and tapes.68 Several studies have demonstrated improved scar quality (ie, scar volume, color, and elasticity, as well as less pain and itching/pruritus) and reduced incidence of hypertrophic and keloid scar formation after silicone-based treatment.68 Despite its widespread use, the exact mechanism of action of this treatment is still not completely understood. It is likely that silicone-based products improve the newly formed epidermis’ barrier function, thus preventing excessive transdermal water loss.69 Dehydration of the epidermis could contribute to pathological scarring by signaling to keratinocytes and fibroblasts to produce excess cytokines and collagen, respectively.69 Other possible mechanisms of action proposed for silicone-based products include minimizing mechanical wound tension, reducing scar vascularity, and generating static electricity through friction, which assists with collagen alignment.69 Silicone-based treatments require long-term use (± 23 hours a day for 6-12 months) to obtain the desired outcome, which often affects patient adherence.69 Although treatment with silicone sheets is generally well-tolerated, issues with skin rashes, pruritus, and skin maceration have been reported, especially in hot or humid climates.70 Silicone gel treatments have several advantages compared to silicone sheets, including reduced visibility, suitability for sensitive skin (less chance of skin irritation), and application to large scar areas (eg, burn wounds) and areas that require flexibility (eg, joints).68
Pressure garments. Pressure garments are another widely used, non-invasive method for pathological scar prevention and treatment. Pressure garment therapy is routinely indicated for use in burn patients to prevent hypertrophic scarring; it is also used for keloid scars.71,72 It is hypothesized that the mechanical pressure exerted by these garments have 2 main effects on scar tissue. First, the mechanical pressure restricts blood flow to the area and induces localized hypoxia (low levels of oxygen), resulting in fibroblast apoptosis and reduced collagen production.71 Second, the constant pressure assists with proper remodeling and alignment of collagen fibers.71 Despite routine use, clinical data on the efficacy of pressure garment therapy is limited and inconsistent.71 The optimal pressure required for therapeutic benefit is also still unknown, although pressure of 15 mm Hg to 25 mm Hg is generally recommended.71 Pressure garment therapy is a long-term treatment option and requires consistent wear until scar maturation has occurred (± 23 hours per day for 6-12 months).71 Unfortunately, this leads to poor patient adherence and drastically reduces the treatment efficacy.71
Minimally invasive treatments
Corticosteroids. Corticosteroids (eg, dexamethasone, methylprednisolone, and triamcinolone) have become standard therapy for the treatment of keloids and hypertrophic scars.73 Corticosteroids are mainly injected directly into the scar tissue (ie, intralesional injections) because topical application is not effective in preventing and treating hypertrophic and keloid scars.73 Their mechanism of action involves reducing inflammation and inhibiting fibroblast activity, which in turn reduces ECM and collagen synthesis.73 Overall, hypertrophic scars are more responsive to corticosteroid treatment than keloid scars. Keloids treated with corticosteroid monotherapy have a high recurrence rate.74 Thus, corticosteroids are used as adjuvant therapy for keloid treatment, often in combination with surgical excision. Despite promising results for scar treatment, corticosteroid therapy requires multiple treatment sessions and is associated with several adverse effects, including pain at the injection site, pruritus, thinning of the skin (skin atrophy), dilated or broken blood vessels (ie, “spider veins” or telangiectasia), and dyspigmentation.73
Chemotherapeutic drugs. Intralesional injection of low-dose chemotherapy drugs (eg, 5-fluorouracil, bleomycin, and mitomycin C) is another adjunctive therapy used mainly for keloid scars.74,75 Due to regression of hypertrophic scars over time, chemotherapeutic drugs are not routinely used because their adverse effects may outweigh their possible benefits.75 Chemotherapeutic drugs are often used in conjunction with intralesional corticosteroid injections and surgical excision to treat and prevent keloid recurrence.75 The exact mechanism of action of these drugs is still unclear, however, in vitro and in vivo studies have shown inhibition of fibroblast proliferation and reduced collagen synthesis.67,74 Although chemotherapeutic drugs are generally well tolerated over a short period, common adverse effects include pain at the injection site, dyspigmentation, and skin ulceration.74,75
Cryotherapy. Cryotherapy, also known as cryosurgery or cryoablation, involves the use of a cryogen (eg, liquid nitrogen) to freeze abnormal/scar tissue (primarily used for keloid scars).76 The freeze/thaw cycle of this technique causes damage to cells and blood vessels of the abnormal tissue and stimulates an immunological response through the release of cytokines from damaged cells.76 Three different methods of cryotherapy exist: spray, contact, and intralesional cryotherapy. For spray and contact cryotherapy, the cryogen is applied directly to the surface of the target lesion by means of a spray nozzle or cryoprobe.76 For intralesional cryotherapy, a cryoneedle is used which is inserted into the core of the target lesion. Intralesional cryotherapy allows targeted freezing of the lesion from the core outwards, minimizing damage to the surrounding skin and reducing the risk of dyspigmentation in patients with darker skin tones.76,77 Compared to contact cryotherapy, intralesional cryotherapy has demonstrated better efficacy with greater scar volume reduction, fewer treatment sessions, and less adverse effects.77
Laser treatments. Laser therapy or laser skin resurfacing is frequently used in the field of dermatology to improve the appearance of both hypertrophic and keloid scars.78 Lasers are classified as either ablative or non-ablative. Non-ablative skin resurfacing with pulsed dye lasers and neodymium-doped yttrium aluminum garnet lasers is a minimally invasive technique that delivers a specific wavelength of light to the dermal layer of the skin without damaging the epidermis.79 The laser causes thermal injury to the dermis, which in turn stimulates the production of collagen and elastin.79 In contrast, ablative skin resurfacing with carbon dioxide lasers and erbium-doped yttrium aluminum garnet lasers is a more invasive technique in which thermal energy removes the epidermal skin layer to reach the dermis.79 Although ablative resurfacing is more effective and requires fewer treatment sessions than non-ablative resurfacing, recovery time is significantly longer and the risk of adverse effects is higher.79 Both ablative and non-ablative lasers exist in fractionated and non-fractionated forms. Non-fractional or full-field laser therapy is the more aggressive option and treats the entire target area.80 Fractional laser therapy only treats certain portions of the target area while leaving some skin uninjured to promote faster re-epithelialization.80 Fractional laser therapy is often used for laser-assisted dermal drug delivery, as it creates microscopic channels that allow topical drugs to penetrate the epidermal barrier.78
Invasive treatments: scar resurfacing
Apart from ablative laser resurfacing, other methods of skin resurfacing include surgical excision and radiotherapy.81 The primary goal of these techniques is to improve the appearance and functionality of scar tissue. This involves disruption of the epidermis, reducing the volume of scar tissue and stimulating the subsequent healing process.81
Surgical intervention can range from reducing the scar volume (eg, shaving of the skin surface by means of sharp dissection) to complete scar excision.81 Depending on the depth of tissue removed, skin flaps, grafts, or skin substitutes may be required to cover the wound after surgery.82 Z- and W-plasties are wound closure techniques used to relieve contraction and create a less conspicuous scar by realigning it with the resting tension lines of the skin.83 Hypertrophic scars do not always require surgical intervention due to spontaneous regression over time. However, excisional debulking followed by low-tension wound closure, as mentioned above, is often used to improve the appearance of pre-existing hypertrophic scars.84 Surgical excision is also indicated in cases where hypertrophic scar contractures (especially around the joints) result in loss of function. Keloid scars often require surgical intervention, especially in cases where these scars are unresponsive to other treatment options. However, due to the high risk of keloid recurrence, subsequent adjunctive therapies are required after excision.82 Studies have shown that excision used in combination with radiotherapy significantly decreased the keloid recurrence rate.82 During radiotherapy, the lesion is either subjected to an external radiation source (external beam radiation therapy) or the radiation source is implanted inside or adjacent to the lesion (brachytherapy).82,85 Brachytherapy has several advantages compared to external beam radiation therapy, including localized radiation delivery, less damage to surrounding tissues, fewer treatment sessions, and less adverse effects.85 Adverse effects associated with radiotherapy include redness of the skin (erythema), telangiectasia, dyspigmentation, and wound-related complications (eg, wound dehiscence).85
Conclusion
Effective treatment of chronic wounds and abnormal scars remains challenging. Although various treatment options are available for both, including several promising new therapies, there are limitations that still need to be addressed. Due to the complexity of chronic wounds and aberrant scars, treatment must be adapted to each individual patient to obtain optimal results. As there is currently no universal treatment regimen, the choice of treatment method is primarily based on the health care professional’s experience and preference. Many of these treatment procedures also lack a standardized protocol, which significantly affects reproducibility and clinical outcome.
Scientific evidence regarding the efficacy and safety of most aesthetic procedures is limited, and their mechanisms of action are still unknown. The molecular mechanisms responsible for chronic wound and pathological scar formation and recurrence, as well as the factors involved in healing and prevention, have not been fully elucidated. There is therefore an urgent need for high-quality scientific research addressing these topics.
Acknowledgments
Authors: Chantalle Crous, PhD1; Judey Pretorius, PhD2; and Anél Petzer, PhD1,3
Affiliations: 1Centre of Excellence for Pharmaceutical Sciences, North-West University, Potchefstroom, South Africa; 2Biomedical Emporium, Pretoria, South Africa; 3Pharmaceutical Chemistry, School of Pharmacy, North-West University, Potchefstroom, South Africa
ORCID: Crous, 0000-0002-5603-4328
Disclosures: Dr. Pretorius is the director of Biomedical Emporium. The remaining authors have no financial or other conflicts of interest to disclose.
Funding: Financial support was provided by Biomedical Emporium.
Correspondence: Chantalle Crous, PhD; Centre of Excellence for Pharmaceutical Sciences, North-West University, Potchefstroom 2520, South Africa; 21204756@mynwu.ac.za
References
1. Ellis S, Lin EJ, Tartar D. Immunology of wound healing. Curr Dermatol Rep. 2018;7(4):350-358. doi:10.1007/s13671-018-0234-9
2. Raina N, Rani R, Pahwa R, Gupta M. Biopolymers and treatment strategies for wound healing: an insight view. Int J Polym Mater. 2020;71(5):359-375. doi:10.1080/00914037.2020.1838518
3. Moore AL, Marshall CD, Barnes LA, Murphy MP, Ransom RC, Longaker MT. Scarless wound healing: transitioning from fetal research to regenerative healing. Wiley Interdiscip Rev Dev Biol. 2018;7(2):10.1002/wdev.309. doi:10.1002/wdev.309
4. Chen Y, Zhong H, Zhao Y, Luo X, Gao W. Role of platelet biomarkers in inflammatory response. Biomark Res. 2020;8:28. doi:10.1186/s40364-020-00207-2
5. D’Arpa P, Leung KP. Toll-like receptor signaling in burn wound healing and scarring. Adv Wound Care (New Rochelle). 2017;6(10):330-343. doi:10.1089/wound.2017.0733
6. El-Zayat SR, Sibaii H, Mannaa FA. Toll-like receptors activation, signaling, and targeting: an overview. Bulletin of the National Research Centre. 2019;43(1):187. doi:10.1186/s42269-019-0227-2
7. Raziyeva K, Kim Y, Zharkinbekov Z, Kassymbek K, Jimi S, Saparov A. Immunology of acute and chronic wound healing. Biomolecules. 2021;11(5):700. doi:10.3390/biom11050700
8. Landén NX, Li D, Ståhle M. Transition from inflammation to proliferation: a critical step during wound healing. Cell Mol Life Sci. 2016;73(20):3861-3885. doi:10.1007/s00018-016-2268-0
9. Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care (New Rochelle). 2015;4(9):560-582. doi:10.1089/wound.2015.0635
10. Guo S, Dipietro LA. Factors affecting wound healing. J Dent Res. 2010;89(3):219-229. doi:10.1177/0022034509359125
11. Ganesh GV, Ramkumar KM. Macrophage mediation in normal and diabetic wound healing responses. Inflamm Res. 2020;69(4):347-363. doi:10.1007/s00011-020-01328-y
12. Wilgus TA, Roy S, McDaniel JC. Neutrophils and wound repair: positive actions and negative reactions. Adv Wound Care (New Rochelle). 2013;2(7):379-388. doi:10.1089/wound.2012.0383
13. Krishnaswamy VR, Mintz D, Sagi I. Matrix metalloproteinases: the sculptors of chronic cutaneous wounds. Biochim Biophys Acta Mol Cell Res. 2017;1864(11 Pt B):2220-2227. doi:10.1016/j.bbamcr.2017.08.003
14. Sabino F, auf dem Keller U. Matrix metalloproteinases in impaired wound healing. Metalloproteinases in Medicine. 2015;2:1-8. doi:10.2147/MNM.S68420
15. Tomic-Canic M, DiPietro LA. Cellular senescence in diabetic wounds: when too many retirees stress the system. J Invest Dermatol. 2019;139(5):997-999. doi:10.1016/j.jid.2019.02.019
16. Wilkinson HN, Clowes C, Banyard KL, Matteuci P, Mace KA, Hardman MJ. Elevated local senescence in diabetic wound healing is linked to pathological repair via CXCR2. J Invest Dermatol. 2019;139(5):1171-1181.e6. doi:10.1016/j.jid.2019.01.005
17. Worsley AL, Lui DH, Ntow-Boahene W, Song W, Good L, Tsui J. The importance of inflammation control for the treatment of chronic diabetic wounds. Int Wound J. 2023;20(6):2346-2359. doi:10.1111/iwj.14048
18. Mendoza RA, Hsieh J, Galiano RD. The impact of biofilm formation on wound healing. In: Dogan KH, ed. Wound Healing - Current Perspectives. IntechOpen; 2019. doi:10.5772/intechopen.85020
19. Zhao R, Liang H, Clarke E, Jackson C, Xue M. Inflammation in chronic wounds. Int J Mol Sci. 2016;17(12):2085. doi:10.3390/ijms17122085
20. Limandjaja GC, Niessen FB, Scheper RJ, Gibbs S. Hypertrophic scars and keloids: overview of the evidence and practical guide for differentiating between these abnormal scars. Exp Dermatol. 2021;30(1):146-161. doi:10.1111/exd.14121
21. Alster TS, Tanzi EL. Hypertrophic scars and keloids: etiology and management. Am J Clin Dermatol. 2003;4(4):235-243. doi:10.2165/00128071-200304040-00003
22. Glass DA II. Current understanding of the genetic causes of keloid formation. J Investig Dermatol Symp Proc. 2017;18(2):S50-S53. doi:10.1016/j.jisp.2016.10.024
23. Ogawa R. Mechanobiology of cutaneous scarring. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:11-18.
24. Limandjaja GC, Belien JM, Scheper RJ, Niessen FB, Gibbs S. Hypertrophic and keloid scars fail to progress from the CD34- /α-smooth muscle actin (α-SMA)+ immature scar phenotype and show gradient differences in α-SMA and p16 expression. Br J Dermatol. 2020;182(4):974-986. doi:10.1111/bjd.18219
25. Karppinen SM, Heljasvaara R, Gullberg D, Tasanen K, Pihlajaniemi T. Toward understanding scarless skin wound healing and pathological scarring. F1000Res. 2019;8:F1000 Faculty Rev-787. doi:10.12688/f1000research.18293.1
26. Xue M, Jackson CJ. Extracellular matrix reorganization during wound healing and its impact on abnormal scarring. Adv Wound Care (New Rochelle). 2015;4(3):119-136. doi:10.1089/wound.2013.0485
27. Ogawa R. Keloid and hypertrophic scars are the result of chronic inflammation in the reticular dermis. Int J Mol Sci. 2017;18(3):606. doi:10.3390/ijms18030606
28. Shirakami E, Yamakawa S, Hayashida K. Strategies to prevent hypertrophic scar formation: a review of therapeutic interventions based on molecular evidence. Burns Trauma. 2020;8:tkz003. doi:10.1093/burnst/tkz003
29. Kumta S, Ritz M, Hurley JV, Crowe D, Romeo R, O’Brien BM. Acute inflammation in foetal and adult sheep: the response to subcutaneous injection of turpentine and carrageenan. Br J Plast Surg. 1994;47(5):360-368. doi:10.1016/0007-1226(94)90096-5
30. Oztürk S, Deveci M, Sengezer M, Günhan O. Results of artificial inflammation in scarless foetal wound healing: an experimental study in foetal lambs. Br J Plast Surg. 2001;54(1):47-52. doi:10.1054/bjps.2000.3460
31. Wilgus TA. Inflammation as an orchestrator of cutaneous scar formation: a review of the literature. Plast Aesthet Res. 2020;7:54. doi:10.20517/2347-9264.2020.150
32. Martin P, D’Souza D, Martin J, et al. Wound healing in the PU.1 null mouse--tissue repair is not dependent on inflammatory cells. Curr Biol. 2003;13(13):1122-1128. doi:10.1016/s0960-9822(03)00396-8
33. Wang Z-C, Zhao W-Y, Cao Y, et al. The roles of inflammation in keloid and hypertrophic scars. Front Immunol. 2020;11:603187. doi:10.3389/fimmu.2020.603187
34. Nguyen JK, Austin E, Huang A, Mamalis A, Jagdeo J. The IL-4/IL-13 axis in skin fibrosis and scarring: mechanistic concepts and therapeutic targets. Arch Dermatol Res. 2020;312(2):81-92. doi:10.1007/s00403-019-01972-3
35. Ferreira AM, Takagawa S, Fresco R, Zhu X, Varga J, DiPietro LA. Diminished induction of skin fibrosis in mice with MCP-1 deficiency. J Invest Dermatol. 2006;126(8):1900-1908. doi:10.1038/sj.jid.5700302
36. Nishiguchi MA, Spencer CA, Leung DH, Leung TH. Aging suppresses skin-derived circulating SDF1 to promote full-thickness tissue regeneration. Cell Rep. 2018;24(13):3383-3392.e5. doi:10.1016/j.celrep.2018.08.054
37. Fujita M, Yamamoto Y, Jiang JJ, et al. NEDD4 is involved in inflammation development during keloid formation. J Invest Dermatol. 2019;139(2):333-341. doi:10.1016/j.jid.2018.07.044
38. Makino S, Mitsutake N, Nakashima M, et al. DHMEQ, a novel NF-kappaB inhibitor, suppresses growth and type I collagen accumulation in keloid fibroblasts. J Dermatol Sci. 2008;51(3):171-180. doi:10.1016/j.jdermsci.2008.03.003
39. Lim CP, Phan TT, Lim IJ, Cao X. Stat3 contributes to keloid pathogenesis via promoting collagen production, cell proliferation and migration. Oncogene. 2006;25(39):5416-5425. doi:10.1038/sj.onc.1209531
40. Ray S, Ju X, Sun H, Finnerty CC, Herndon DN, Brasier AR. The IL-6 trans-signaling-STAT3 pathway mediates ECM and cellular proliferation in fibroblasts from hypertrophic scar. J Invest Dermatol. 2013;133(5):1212-1220. doi:10.1038/jid.2012.499
41. Dohi T, Padmanabhan J, Akaishi S, et al. The interplay of mechanical stress, strain, and stiffness at the keloid periphery correlates with increased caveolin-1/ROCK signaling and scar progression. Plast Reconstr Surg. 2019;144(1):58e-67e. doi:10.1097/prs.0000000000005717
42. Wong VW, Rustad KC, Akaishi S, et al. Focal adhesion kinase links mechanical force to skin fibrosis via inflammatory signaling. Nat Med. 2011;18(1):148-152. doi:10.1038/nm.2574
43. Honardoust D, Varkey M, Hori K, Ding J, Shankowsky HA, Tredget EE. Small leucine-rich proteoglycans, decorin and fibromodulin, are reduced in postburn hypertrophic scar. Wound Repair Regen. 2011;19(3):368-378. doi:10.1111/j.1524-475X.2011.00677.x
44. Pang X, Dong N, Zheng Z. Small leucine-rich proteoglycans in skin wound healing. Front Pharmacol. 2020;10:1649. doi:10.3389/fphar.2019.01649
45. Potekaev NN, Borzykh OB, Medvedev GV, et al. The role of extracellular matrix in skin wound healing. J Clin Med. 2021;10(24):5947. doi:10.3390/jcm10245947
46. Moore Z, Dowsett C, Smith G, et al. TIME CDST: an updated tool to address the current challenges in wound care. J Wound Care. 2019;28(3):154-161. doi:10.12968/jowc.2019.28.3.154
47. Leaper DJ, Schultz G, Carville K, Fletcher J, Swanson T, Drake R. Extending the TIME concept: what have we learned in the past 10 years? Int Wound J. 2012;9(Suppl 2):1-19. doi:10.1111/j.1742-481X.2012.01097.x
48. Goswami AG, Basu S, Banerjee T, Shukla VK. Biofilm and wound healing: from bench to bedside. Eur J Med Res. 2023;28(1):157. doi:10.1186/s40001-023-01121-7
49. Schultz G, Bjarnsholt T, James GA, et al; Global Wound Biofilm Expert Panel. Consensus guidelines for the identification and treatment of biofilms in chronic nonhealing wounds. Wound Repair Regen. 2017;25(5):744-757. doi:10.1111/wrr.12590
50. Percival SL, Mayer D, Kirsner RS, et al. Surfactants: role in biofilm management and cellular behaviour. Int Wound J. 2019;16(3):753-760. doi:10.1111/iwj.13093
51. Percival SL, Chen R, Mayer D, Salisbury AM. Mode of action of poloxamer-based surfactants in wound care and efficacy on biofilms. Int Wound J. 2018;15(5):749-755. doi:10.1111/iwj.12922
52. Das Ghatak P, Mathew-Steiner SS, Pandey P, Roy S, Sen CK. A surfactant polymer dressing potentiates antimicrobial efficacy in biofilm disruption. Sci Rep. 2018;8(1):873. doi:10.1038/s41598-018-19175-7
53. Alves PJ, Barreto RT, Barrois BM, Gryson LG, Meaume S, Monstrey SJ. Update on the role of antiseptics in the management of chronic wounds with critical colonisation and/or biofilm. Int Wound J. 2021;18(3):342-358. doi:10.1111/iwj.13537
54. Jeong S, Schultz GS, Gibson DJ. Testing the influence of surfactant-based wound dressings on proteinase activity. Int Wound J. 2017;14(5):786-790. doi:10.1111/iwj.12697
55. Wright JB, Lam K, Buret AG, Olson ME, Burrell RE. Early healing events in a porcine model of contaminated wounds: effects of nanocrystalline silver on matrix metalloproteinases, cell apoptosis, and healing. Wound Repair Regen. 2002;10(3):141-151. doi:10.1046/j.1524-475x.2002.10308.x
56. Serra R, Gallelli L, Buffone G, et al. Doxycycline speeds up healing of chronic venous ulcers. Int Wound J. 2015;12(2):179-184. doi:10.1111/iwj.12077
57. Xu DH, Zhu Z, Fang Y. The effect of a common antibiotics doxycycline on non-healing chronic wound. Curr Pharm Biotechnol. 2017;18(5):360-364. doi:10.2174/1389201018666170519095339
58. McCarty SM, Percival SL. Proteases and delayed wound healing. Adv Wound Care (New Rochelle). 2013;2(8):438-447. doi:10.1089/wound.2012.0370
59. Jones RE, Foster DS, Longaker MT. Management of chronic wounds-2018. JAMA. 2018;320(14):1481-1482. doi:10.1001/jama.2018.12426
60. Vowden K, Vowden P. Wound dressings: principles and practice. Surgery (Oxford). 2017;35(9):489-494. doi:10.1016/j.mpsur.2017.06.005
61. Suissa D, Danino A, Nikolis A. Negative-pressure therapy versus standard wound care: a meta-analysis of randomized trials. Plast Reconstr Surg. 2011;128(5):498e-503e. doi:10.1097/PRS.0b013e31822b675c
62. Serena TE, Jalodi O, Serena L, Patel K, Mynti M. Evaluation of the combination of a biofilm-disrupting agent and negative pressure wound therapy: a case series. J Wound Care. 2021;30(1):9-14. doi:10.12968/jowc.2021.30.1.9
63. Tahir S, Malone M, Hu H, Deva A, Vickery K. The effect of negative pressure wound therapy with and without instillation on mature biofilms in vitro. Materials (Basel). 2018;11(5):811. doi:10.3390/ma11050811
64. Dai C, Shih S, Khachemoune A. Skin substitutes for acute and chronic wound healing: an updated review. J Dermatolog Treat. 2020;31(6):639-648. doi:10.1080/09546634.2018.1530443
65. Timmermans FW, Middelkoop E. Invasive techniques in scar management: skin substitutes. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:317-323.
66. Tan SH, Ngo ZH, Sci DB, Leavesley D, Liang K. Recent advances in the design of three-dimensional and bioprinted scaffolds for full-thickness wound healing. Tissue Eng Part B Rev. 2022;28(1):160-181. doi:10.1089/ten.TEB.2020.0339
67. Elsaie ML. Update on management of keloid and hypertrophic scars: a systemic review. J Cosmet Dermatol. 2021;20(9):2729-2738. doi:10.1111/jocd.14310
68. Mustoe TA. Evolution of silicone therapy and mechanism of action in scar management. Aesthetic Plast Surg. 2008;32(1):82-92. doi:10.1007/s00266-007-9030-9
69. Bleasdale B, Finnegan S, Murray K, Kelly S, Percival SL. The use of silicone adhesives for scar reduction. Adv Wound Care (New Rochelle). 2015;4(7):422-430. doi:10.1089/wound.2015.0625
70. Nikkonen MM, Pitkanen JM, Al-Qattan MM. Problems associated with the use of silicone gel sheeting for hypertrophic scars in the hot climate of Saudi Arabia. Burns. 2001;27(5):498-501. doi:10.1016/s0305-4179(01)00004-3
71. Ai JW, Liu JT, Pei SD, et al. The effectiveness of pressure therapy (15-25 mmHg) for hypertrophic burn scars: a systematic review and meta-analysis. Sci Rep. 2017;7:40185. doi:10.1038/srep40185
72. Ojeh N, Bharatha A, Gaur U, Forde AL. Keloids: current and emerging therapies. Scars Burn Heal. 2020;6:2059513120940499. doi:10.1177/2059513120940499
73. Lee J, Kim J. Minimal-invasive technologies for treatment of HTS and keloids: corticosteroids. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:243-250.
74. Jones CD, Guiot L, Samy M, Gorman M, Tehrani H. The use of chemotherapeutics for the treatment of keloid scars. Dermatol Reports. 2015;7(2):5880. doi:10.4081/dr.2015.5880
75. Liu W, Wu X, Gao Z, Xia L. Minimally invasive technologies for treatment of HTS and keloids: low-dose 5-fluorouracil. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:251-262.
76. Krunic AL, Marini LG. Cryosurgery. In: Katsambas AD, Lotti TM, Dessinioti C, D’Erme AM, eds. European Handbook of Dermatological Treatments. 3rd ed. Springer Berlin Heidelberg; 2015:1139-1149.
77. Har-Shai Y, Har-Shai L. Minimally invasive technologies for the treatment of hypertrophic scars and keloids: intralesional cryosurgery. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:235-241.
78. Searle T, Ali FR, Al-Niaimi F. Lessons learned from the first decade of laser-assisted drug delivery. Dermatol Ther (Heidelb). 2021;11(1):93-104. doi:10.1007/s13555-020-00478-5
79. Preissig J, Hamilton K, Markus R. Current laser resurfacing technologies: a review that delves beneath the surface. Semin Plast Surg. 2012;26(3):109-116. doi:10.1055/s-0032-1329413
80. Yumeen S, Khan T. Laser-Erbium-Yag Resurfacing. Updated July 10, 2023. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK560931/
81. Wood FM. Scar resurfacing. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:311-316.
82. Dong W, Qiu B, Fan F. Adjuvant radiotherapy for keloids. Aesthetic Plast Surg. 2022;46(1):489-499. doi:10.1007/s00266-021-02442-w
83. Shockley WW. Scar revision techniques: z-plasty, w-plasty, and geometric broken line closure. Facial Plast Surg Clin North Am. 2011;19(3):455-463. doi:10.1016/j.fsc.2011.06.002
84. Mony MP, Harmon KA, Hess R, Dorafshar AH, Shafikhani SH. An updated review of hypertrophic scarring. Cells. 2023;12(5):678. doi:10.3390/cells12050678
85. de Bakker E, van Leeuwen MCE, Meijer OWM, Niessen FB. Additional invasive techniques in scar management. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, eds. Textbook on Scar Management: State of the Art Management and Emerging Technologies. 1st ed. Springer; 2020:343-349.
