


Charcot Foot Deformity: Surgical Treatment Options
With longer survival rates of patients with diabetes the incidence of Charcot arthropathy has been noted to be increasing in occurrence within the last several years.1 Charcot arthropathy is a noninfective progressive process that was first reported by Jean-Martin Charcot in 1868.2 It was originally described in neuropathic patients with tertiary syphilis, although it is now most commonly associated with diabetes mellitus. It has also been associated with peripheral neuropathy caused by alcoholism, syringomyelia, rheumatoid arthritis, leprosy, multiple sclerosis, and trauma. It has been reported that 30%–50% of patients with diabetes have neuropathy, but only 0.2%–2.5% will develop Charcot arthropathy.3
Charcot arthropathy is usually characterized by painless joint destruction, fracture, and eventual dislocation. Men and women are equally affected, and it occurs bilaterally in 30% of cases.4 The exact etiology remains controversial, but two main theories exist.
Charcot proposed the neurovascular theory stating that the cause was the damaged trophic centers of the spine that control bone and joint nutrition, resulting in a neurally initiated increase of blood flow to bone;5 this is known as the French theory. The neurotraumatic theory, or German theory, proposed by Volkmann and Virchow, states that decreased protective sensation allows repetitive trauma to result in fracture and dislocation.6 Continued weight bearing causes mechanical failure and collapse. Indeed it is a commonly held opinion that the etiology is most likely a combination of both.
Clinical Evaluation
Clinically, the acute Charcot foot usually presents with erythema, edema, and varying degrees of loss of protective sensation. It is often mistaken for cellulitis. Laboratory tests, radiographs, and clinical suspicion may help rule this out. Often, elevating the involved extremity for 10 minutes may provide a way to help distinguish between edema associated with infection versus Charcot changes, as swelling associated with infection will often remain.7 Edema that subsides with elevation may be more indicative of Charcot arthropathy.
When ordering radiographs, it is best to image the foot and ankle in a weight bearing position to evaluate the stage of deformity and biomechanical malalignments including plantar prominences. Further diagnostic imaging may be needed to help rule out infection. Magnetic resonance imaging may be helpful when looking for abscess and when evaluating for osteomyelitis. Possibly the best imaging tool available to help distinguish between osteomyelitis and Charcot arthropathy is an indium-labeled white blood cell scan.8
It is important to evaluate all patients for Achilles tendon contracture who present with a possible diabetic Charcot foot. Achilles tendon contracture may lead to increased plantar foot pressures, in particular across the plantar forefoot and midfoot.9 Increased plantar pressures may lead to soft tissue compromise and ulceration. Ankle equinus deformity must be corrected to alleviate these stresses.
Charcot Foot Staging
Staging of the Charcot foot has been based primarily on radiographic analysis and anatomic site. In 1966, Eikenholtz was probably the first to classify the radiographic and clinical changes associated with charcot arthropathy.10 Stage 1 is characterized by the development of an erythematous and edematous foot. There is usually radiographic evidence of subluxation, dislocation, or joint disruption along with bone fragmentation. Stage 2, or the “coalescence phase,” is characterized by decreasing erythema, warmth, and edema. Fracture healing occurs and sclerotic changes may be seen in the juxta-articular bone surfaces. In stage 3, reconstructive and consolidation changes occur. Many times the deformity will become fixed and stable during this phase.
In 1993, Brodsky and Rouse11 described an anatomic classification consisting of 3 main types with further sub-classification. Type I deformity is the most common (60%–70%) and is described as changes involving the midfoot. Type II changes, or those located in the hindfoot, primarily involve the subtalar joint complex and occurs in 20%–25% of cases. Type III changes are the least common (10%–15%) and are split into 2 subgroups. Type IIIa primarily involves the tibiotalar joint complex and leads to the most severe instability that often contributes to breakdown and ulceration. Type IIIb is a pathologic fracture of the tubercle of the os calcis (heel bone) and may result in a pes planus (flat foot) deformity and/or Achilles tendon insufficiency.
Treatment Options
The treatment of the Charcot foot involves both nonoperative and operative measures. The choice of either depends on the severity of the problem and degree of deformity present, presence or absence of ulceration and/or infection, duration of the Charcot process, and history of previous treatment. Nonoperative treatment includes the use of a total contact cast not only for immobilization but also to distribute pressure and control edema. A Charcot Restraint Orthotic Walker or prefabricated pneumatic ambulatory walker may also be utilized.12 The duration of immobilization for Charcot arthropathy may range from a few to many months with a large proportion of this being completely non-weight bearing. Once the extremity is stabilized the patient can then be managed with custom total contact orthotics, protective bracing and/or accommodative or custom-molded shoewear.
Unfortunately, even when the patient is treated appropriately with immobilization and offloading, progression to deformity may still occur. Chronic varus or valgus foot and/or ankle deformity may result. Midfoot collapse and rocker bottom deformity may also occur, with or without ulceration. If there is progression to nonbraceable deformity or nonhealing ulceration despite adequate wound care, operative treatment is then entertained.
Many obvious challenges may be associated with surgery in this patient population (eg, comorbidities such as impaired renal and cardiac function, poor nutritional status, immunopathy). Proper preoperative evaluation, often by a multidisciplinary team of specialists, is critical as well as the assurance of the necessary vascular perfusion to achieve healing. Surgical options include exostectomy and reconstruction, with or without various plastic surgical procedures (which may help with wound closure) and amputation, which should be reserved for only the nonsalvegable extremity.
Surgical Treatment Options
Exostectomy. If an osseous prominence is present with or without ulceration in an otherwise plantigrade foot, removal of the prominence via exostectomy may be a treatment alternative. In the presence of an Achilles tendon contracture, a concurrent Achilles tendon lengthening is performed. Plantar or posterior prominences may be present, although plantar prominences are much more frequent. Most plantar prominences will be based laterally but they are also occasionally seen medially. The surgical approach may involve a lateral or medial off weight-bearing incision or may involve a direct plantar approach with excision of the ulceration. At times various forms of rotation or advancement flaps may be used to augment wound closure and exposure. The osseous prominence is then resected and the area is smoothed. Intra-operative cultures are performed in the presence of ulceration. Postoperative care involves varying lengths of immobilization and off weight bearing depending on the incisional approach used, with plantar incisions or flaps usually requiring longer periods of non-weight bearing. Postoperative immobilization techniques include removable cam-type boots that allow for dressing changes and wound inspection. Long-term care may include the use of orthotic bracing and accommodative or custom shoewear. A retrospective study has reported on the success rate of exostectomy.13
Reconstruction. Indications for surgical reconstruction or realignment procedures include unbraceable situations and/or chronic nonhealing ulcerations resulting from varus or valgus deformities and contractures. Some acute fractures of the foot and ankle are also indications for reconstructive procedures. As in exostectomy, an Achilles tendon lengthening may also be required as well as plastic surgical techniques for wound coverage. Surgical goals are to resect and smooth osseous prominences, correct deformity, and achieve a stable plantigrade foot. In most cases of deformity correction, one or more joints are arthrodesed. Although ideally solid bony fusion is sought, a stable fibrous nonunion without deformity may be acceptable. If possible, surgical reconstruction is preferably carried out after healing of any ulceration that may be present.14 Unfortunately, deformity correction may need to be performed first to offload the affected area and allow the ulceration healing to proceed. Reconstructive surgery on the Charcot foot can be challenging and complications may be more frequent than with exostectomy. However, with proper patient selection, surgical reconstruction has been shown to be effective in a high percentage of patients, resulting in limb salvage.15
Both internal fixation and external fixation may be used in the surgical reconstruction of the Charcot foot deformity. Rates of union after foot and ankle arthrodesis using internal fixation averaged 65%–70%.16 Multiplanar osteotomies used for deformity correction may also be stabilized with internal fixation. Screws, plates, or intramedullary rods are all examples of internal fixation and are used to achieve compression across arthrodesis and osteotomy sites, and to maintain proper foot and ankle alignment.
External fixation techniques are an alternative to internal fixation methods in the surgical reconstruction of the Charcot foot deformity. Excellent fixation and stability has been shown to occur with external fixation in this patient population. Although the modern concept of external fixation has been around since the 1940s, it was not until 1996 that it was advocated for treatment of Charcot arthropathy.17 External fixation can be particularly advantageous in patients with ulceration, infection, or in patients who have failed internal fixation. External fixation methods include circular (ring), monolateral or hybrid configurations. When the deformity occurs at the midtarsal or tarsometatarsal joints, any of the above techniques may be effective. Although all 3 may also be effective at the level of the ankle and/or subtalar joints, a multiple ring construct may be preferred.4 Various postoperative protocols have been described when using external fixators. For circular external fixators, the frame is usually left in place for a total of 2–3 months or until adequate healing is present radiographically at the arthrodesis or osteotomy site(s).
External fixation frames are advantageous over internal fixation in that they can be placed percutaneously, possibly avoiding more extensive soft tissue dissection, which is sometimes necessary for insertion of internal fixation devices. Ulcerations may also be easily assessed and cared for. With external fixation, the surgeon may possibly address multiplanar deformity and perform some correction throughout the postoperative period, secondary to the fact external fixators can provide neutralization and stabilization with adjustable amounts of compression, distraction, rotation, and translation. This may allow some manipulation over time rather than a single stage correction. The most common complication is pin tract infection (5%–100%).18 Other complications include pin breakage and wound dehiscence. In a recent study, complications of circular fixators were associated with younger age (51 years versus 64 years), elevated preoperative glucose (> 220 mg/dL), and higher extremity tourniquet times (> 119 minutes).19 Younger age was attributed to increased physical activity in comparison to older individuals. Edema may also be difficult to control. When edema occurs fluid exits through the pin sites, which can lead to hardware loosening and infection.4 The surgeon must be familiar with areas for safe pin placement and cross sectional anatomy. Improper pin placement can have disabling effects.
Amputation. Elective major amputation may be a reasonable alternative in some situations, but only in those situations deemed unsalvageable or in poorly perfused limbs. Patients with abscess, extensive bone loss, and articular destruction may benefit from Syme’s amputation if the posterior tibial artery is patent.20
Case Reports
Case 1. A 46-year-old woman with diabetes (controlled with oral medication) presented to the authors’ clinic with an 18-month history of a nonhealing ulcer over the posterior calcaneus secondary to exostectomy for an osseous prominence associated with diabetic Charcot hindfoot deformity (Figure 1). The wound had not healed postoperatively despite aggressive medical and local management, including extensive wound care and bracing.  The patient had not been able to wear conventional or diabetic shoe wear for 2 years. Diagnostic imaging showed an area of suspected chronic osteomyelitis at the posterior, superior aspect of the calcaneus. Her previous treating physician had discussed Calcanectomy versus Syme’s amputation with the patient. After evaluation, which included proper vascular work-up, it was determined that the patient was a candidate for debridement and flap coverage. Excision of the ulceration and osseous debridement of infected bone were performed followed by sural artery flap rotation into the remaining soft tissue deficit (Figure 2). Six weeks of intravenous antibiotic coverage was also undertaken. The wound healed uneventfully and has remained closed at the latest follow-up visit of 18 months (Figure 3). The patient has returned to using diabetic shoe wear.
The patient had not been able to wear conventional or diabetic shoe wear for 2 years. Diagnostic imaging showed an area of suspected chronic osteomyelitis at the posterior, superior aspect of the calcaneus. Her previous treating physician had discussed Calcanectomy versus Syme’s amputation with the patient. After evaluation, which included proper vascular work-up, it was determined that the patient was a candidate for debridement and flap coverage. Excision of the ulceration and osseous debridement of infected bone were performed followed by sural artery flap rotation into the remaining soft tissue deficit (Figure 2). Six weeks of intravenous antibiotic coverage was also undertaken. The wound healed uneventfully and has remained closed at the latest follow-up visit of 18 months (Figure 3). The patient has returned to using diabetic shoe wear.
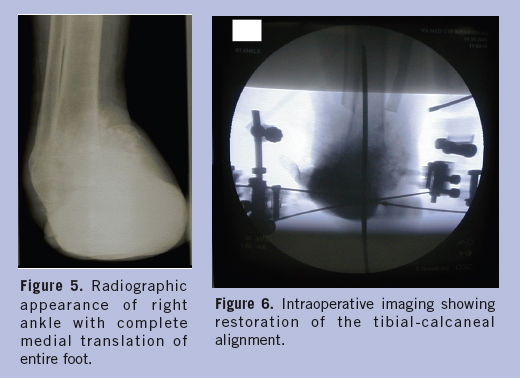
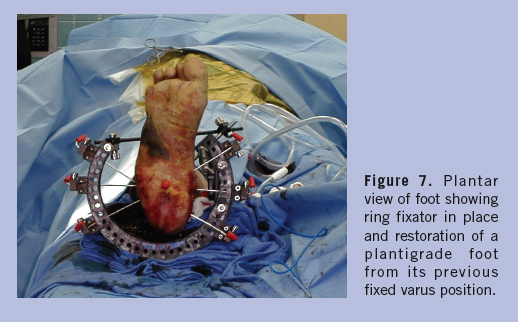
Case 2. A 53-year-old insulin dependent man with diabetes presented to the authors’ clinic with a 3-year history of progressive right foot deformity as a result of diabetic Charcot neuroarthropathy. He had undergone multiple debridements for chronic ulceration and osteomyelitis, including partial fourth and fifth ray resections and split-thickness skin grafting to the lateral aspect of the foot. Examination revealed a fixed varus deformity of the right foot and ankle, nonhealing ulceration over the lateral malleolus, and radiographic evidence of chronic osteomyelitis of the distal fibula, as well as medial talar dislocation (Figures 4 and 5).  Two other specialists had recommended below-knee amputation. The patient was also starting to develop an ulcer on the contralateral foot secondary to gait compensation. After appropriate work-up this patient underwent a resection of the distal fibula and subtotal talectomy with application of a ring fixator for deformity correction and fixation (Figures 6 and 7). The ring fixator was left in place for 31⁄2 months. He ambulated in a Charcot Restraint Orthotic Walker for 5 months following ring fixator removal, and has subsequently returned to diabetic shoe wear and remains ulcer free after 2 years.
Two other specialists had recommended below-knee amputation. The patient was also starting to develop an ulcer on the contralateral foot secondary to gait compensation. After appropriate work-up this patient underwent a resection of the distal fibula and subtotal talectomy with application of a ring fixator for deformity correction and fixation (Figures 6 and 7). The ring fixator was left in place for 31⁄2 months. He ambulated in a Charcot Restraint Orthotic Walker for 5 months following ring fixator removal, and has subsequently returned to diabetic shoe wear and remains ulcer free after 2 years.
 Case 3. A 63-year-old woman with insulin dependent diabetes presented to the authors’ clinic with an 8-month history of nonhealing ulceration on the plantar aspect of the right foot. She had an osseous prominence under the cuboid secondary to diabetic Charcot neuropathic midfoot collapse. Despite aggressive local measures and offloading techniques, the ulceration had failed to heal and had actually progressed in size over the previous 4 months. The patient’s previous treating surgeon had recommended midfoot amputation. Clinical exam showed a contracture of the tendo-Achilles and a grade 2 ulceration that did not probe to bone (Figure 8).
Case 3. A 63-year-old woman with insulin dependent diabetes presented to the authors’ clinic with an 8-month history of nonhealing ulceration on the plantar aspect of the right foot. She had an osseous prominence under the cuboid secondary to diabetic Charcot neuropathic midfoot collapse. Despite aggressive local measures and offloading techniques, the ulceration had failed to heal and had actually progressed in size over the previous 4 months. The patient’s previous treating surgeon had recommended midfoot amputation. Clinical exam showed a contracture of the tendo-Achilles and a grade 2 ulceration that did not probe to bone (Figure 8).  Radiographs showed midfoot Charcot changes and plantar prominence to the cuboid (Figure 9). The foot was otherwise plantigrade and the patient was asymptomatic with excellent vascular status. Due to the failure of nonoperative care, exostectomy (excision of the plantar prominence) was performed (Figures 10 and 11).
Radiographs showed midfoot Charcot changes and plantar prominence to the cuboid (Figure 9). The foot was otherwise plantigrade and the patient was asymptomatic with excellent vascular status. Due to the failure of nonoperative care, exostectomy (excision of the plantar prominence) was performed (Figures 10 and 11). 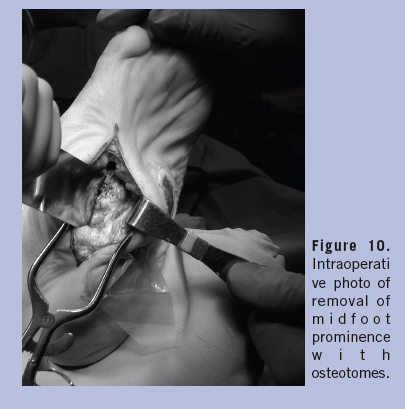 A tendo-Achilles lengthening was also performed. Six weeks after the procedure, the ulceration was closed almost completely (Figure 11). The patient went on to completely heal the ulceration by 9 weeks postoperatively, and remained ulcer free at 2 years post surgery. She ambulates with a custom total contact orthotic and conventional shoe wear.
A tendo-Achilles lengthening was also performed. Six weeks after the procedure, the ulceration was closed almost completely (Figure 11). The patient went on to completely heal the ulceration by 9 weeks postoperatively, and remained ulcer free at 2 years post surgery. She ambulates with a custom total contact orthotic and conventional shoe wear.

Discussion
Major amputation, with below knee amputation being the most common, is often the recommended treatment for the diabetic Charcot foot patient with nonhealing ulceration(s) and/or significant deformity. However, surgical reconstruction remains a treatment alternative in selected individuals (good vascular supply, contained osteomyelitis, etc.). Plastic surgical techniques and newer fixation methods, such as external ring fixation, seem to provide better outcomes and more flexibility in surgical treatment. The main indications for surgery are an unstable deformity, which is not braceable or chronic nonhealing ulceration not responding to nonoperative measures in an adequately perfused foot.
Conclusion
The goal of surgery is to produce an ulceration-free plantigrade foot. Proper orthotic management to hopefully prevent recurrence of problems follows surgery. However, the potential for complications with surgical treatment of the Charcot foot can be high, and can involve eventual limb amputation and death. Excellent surgical planning and preoperative work-up, often by a multidisciplinary team, are crucial to minimize postoperative complications.






