


Clinical Evaluation of Chemical Assault Burns and Occupational Injuries: A 20-year Study at a Single Burn Center
Abstract: Occupational and chemical assault injuries were the two most common factors associated with chemical burns. These two types of injuries were identified and analyzed covering a 20-year period. Methods. Patients with second- to third-degree chemical burns admitted to the Linkou Burn Center, Chang Gung Memorial Hospital from May 1986 to May 2005 were included in the analysis. Injuries other than occupational and chemical assaults were excluded from this study. Results. A total of 46,283 burns were admitted during the study period while 327 patients were included in the study with 250 (77.5%) cases classified to occupational injury (OI) and 77 (23.5%) in the chemical assault (CA) group. The mean age in the OI group was 33.2 years and 36.2 years for the CA group. The mean burn size was 10.9% for the OI group and 14.1% in the CA group. The mean length of hospitalization was 15.8 days in the OI group and 32.3 days in the CA group. The main causative agents were acids, which accounted for 57.2% of injuries in the OI group and 98.7% in the CA group. Sulfuric acid was the primary acidic agent and the main alkali was sodium hydroxide. The face was the most frequently injured area (59.6%) followed by the extremities (upper limb [52.2%], lower limb [44.2%]). The hand injury rate was significantly higher in the OI group (P = 0.009). The injury rates to the face, neck, and chest (P < 0.05) were significantly higher in the CA group. Conclusion. Chemical assault burns might cause more damage and suffering than occupational burn injuries. The promotion of occupational injury protection, public empowerment, and public security in recent years has markedly decreased the occurrence and severity of occupational and chemical-related burns. Modern advances in burn care and surgical procedures contribute greatly to decreasing the length of hospital stays for patients who have sustained an occupational or chemical assault injury. Generally, chemical burn injuries are a result of exposure to acid, alkali, or organic compounds.1 Carelessness is the most common cause of chemical burns, and caution is the most effective form of prevention.2 Cutaneous injury as a result of a chemical burn has greater potential for progressive tissue damage than other types of burn injuries.3 Chemical burns seem to be either much less common or under-referred than other types of burn injuries.4 The etiology of chemical burns varies regarding population, geographical location, surrounding industry, and social environment.4–6  Unlike other countries, occupational injuries and chemical assault injuries in the present survey were the two most common factors associated with chemical burns. The authors’ burn center is located near an industrial park with many factories, and occupational injuries are commonly seen in the authors’ department. Chemical assault injuries are not only unique, but also a common domestic behavior in Taiwan, often as a result of a lovers’ quarrel or arguments over finances. Occupational injuries from a chemical burn have been discussed, but few references in the literature exist regarding chemical assault injuries. Given the unique geographic situation and the large sample size of patients in the authors’ burn center, we have seen many patients with both types of chemical burns. To the best of the authors’ knowledge, a detailed statistical comparison of both injuries has not been undertaken up to this point. Therefore, the authors proceeded to investigate the details of these injuries. The following summarizes the epidemiology and statistical evaluation of patients with chemical assault and occupational chemical injury over a 20-year period.
Unlike other countries, occupational injuries and chemical assault injuries in the present survey were the two most common factors associated with chemical burns. The authors’ burn center is located near an industrial park with many factories, and occupational injuries are commonly seen in the authors’ department. Chemical assault injuries are not only unique, but also a common domestic behavior in Taiwan, often as a result of a lovers’ quarrel or arguments over finances. Occupational injuries from a chemical burn have been discussed, but few references in the literature exist regarding chemical assault injuries. Given the unique geographic situation and the large sample size of patients in the authors’ burn center, we have seen many patients with both types of chemical burns. To the best of the authors’ knowledge, a detailed statistical comparison of both injuries has not been undertaken up to this point. Therefore, the authors proceeded to investigate the details of these injuries. The following summarizes the epidemiology and statistical evaluation of patients with chemical assault and occupational chemical injury over a 20-year period. 
Patients and Methods
The Linkou Burn Center of Chang Gung Memorial Hospital is a 30-bed burn center (the largest burn center in Asia) and receives tertiary referrals from other hospitals. All medical records of patients with a chemical burn admitted to the Burn Center from May 1986 to May 2005 were reviewed. Patients whose injury was identified in the burn registry as other than “accident, employment related” or “assault injury, criminal” were excluded from the present study. In total, 327 patients were included. Basic patient characteristics, length of stay (hospitalization [LOS] days), total burn surface area (TBSA %), operation times, revision surgeries, causative chemicals agents, and occupations were recorded from medical charts. Both groups’ injuries were described using location, injury degree, injury extent, and causative agent(s). The reconstruction implication for both groups, such as split-thickness skin grafts (STSG), full-thickness skin grafts (FTSG), free flaps, and local flaps were also recorded. An independent t test was utilized to highlight any significant differences among injuries. All statistical analyses were performed with SPSS 13.0 (SPSS Institute, Chicago, IL). 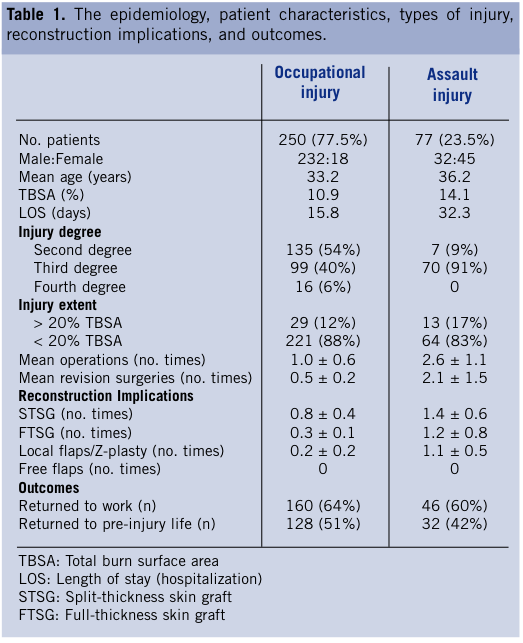
Results
A total of 327 patients with chemical burn injuries covering a 20-year span were included in this study. Two hundred fifty (68.7%) patients were classified in the occupational injury (OI) and 77 (21.2%) cases were included in the chemical assault (CA) group. Comparison of epidemiological data, patient characteristics, LOS, TBSA, mean operation times, mean revision surgeries, injury types, reconstruction implications, and outcomesare presented in Table 1. The OI group had a greater percentage of second-degree burns, while the CA group had more third-degree injuries and more extensive burns. Also, the OI group underwent less revision surgery (local flap or Z-plasty) and seemed to return to work more easily (Table 1). A retro-correlation was discovered for the comparison of occupation. In the OI group, 77.2% of patients were workers and 20% were farmers. Conversely, 45.5% of CA patients were public employees and 29.9% were businessmen (Table 2). The major causative agents were acids in both the OI (57.2%) and CA group (98.7%). The primary acidic agent identified was sulfuric acid and the primary alkali agent was sodium hydroxide. The chemicals responsible for burn injury are reported in Table 3. The most frequently injured area was the face (59.6%) followed by the extremities (upper limb 52.2%, lower limb 44.2%). Further analysis revealed that the hand involvement rate (P ≤ 0.05) was significantly higher in the OI compared to the CA group. The opposite was reflected in the injury rates to the face (P ≤ 0.05), neck (P ≤ 0.05), and chest (P ≤ 0.05), which were significantly higher in the CA group (Table 4). The TBSA in the two groups did not have any obvious differences. However, the LOS remained significantly higher in the CA group. Nevertheless, due to the improvement of medical care, LOS has decreased in recent years. 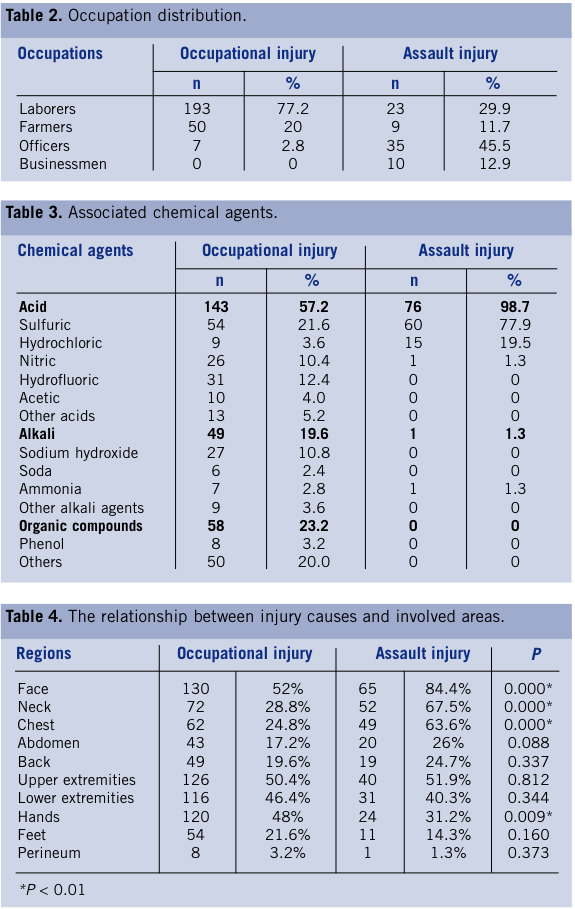
Discussion
Chemical burn injury is defined as a burn injury caused by exposure to an acid, alkali, or organic compound. Chemical burns are much less frequent than other types of burn injuries. The etiology of chemical burns varies depending on the population, geographical location, surrounding industry, and social environment. Violence is a frequent and serious problem in Taiwan, and since guns are now prohibited, organic compounds have become a “weapon.” The reported incidence of assault burn injury ranges from 4% to 13%.7,8 There is wide variability in the global distribution of chemical assault burns dependent upon local industry, social habits, and criminal activity.9 Chemical assault injuries have become a public concern because of the publicity about related factors such as poverty, lovers’ quarrels, and other criminal activities. Occupational burn injuries are most likely to occur at a person’s employment where the worker is exposed to chemicals or other substances. An occupational chemical injury is very hazardous,10,11 not only due to the inherent danger of the toxic materials, but also the physical management of these agents.12 More second-degree (54% vs. 9%) and fourth-degree (6% vs. 0%) burns were seen in the OI group. The number of third-degree burns was higher in the CA group was more than that in the OI group (91% vs. 40%, respectively). As for TBSA, there was no obvious difference between groups. In the authors’ opinion, strong acidic agents, such as sulfuric, hydrochloric, and nitric acids were often used in assault attacks because of an intense revenge motive; therefore, third degree chemical burns were more often seen in the assault injury cases. Hydrofluoric acid, an inherently invasive agent that corrodes bone tissue, was suspected to be the cause of the fourth-degree chemical burns in the OI group. As for the reconstruction implications, not only split-thickness skin graft (STSG), but also full-thickness skin graft (FTSG) and local flaps were more often performed in CA patients. Free flaps were not used in either group to treat injuries. This situation was compatible with the number of mean operation and mean revision surgeries.  Mean burn size was similar between OI and CA, but LOS was doubled in the CA group (Table 1). Additionally, the mean operation time was double, and mean revision surgeries were four-fold higher in the CA group despite improvements in operative and medical care. Patients often required more reconstruction procedures for both functional and cosmetic reasons because the face and neck were often involved. For the same reasons, operation times were longer and revision surgeries more numerous. In the OI group, 64% patients were able to return to work and 51% patients were able to return to their pre-injury life. In the CA group, 60% patients were able to return to work; however, only 42% patients were able to return to their pre-injury life. The hand involvement rate was significantly higher in OI patients, most likely because workers did not use protective rubber gloves while working (Table 4).2 Professional training and occupational injury prevention were generally not sufficient for workers handling chemicals. On the contrary, the injury rates to the face, neck, and chest were significantly higher in the CA group, which is similar to the results reported by Branday et al.9 Fifty-one percent to 60% of patients in both groups had successful primary operations and secondary revisions to their hands and were able to return to work. Conversely, even after satisfactory reconstruction and further revisions for face and neck, only 42% of CA patients were able to return to their pre-injury life; the explanation for this seems to be the social stigma attached to such an injury. Therefore, in the authors’ opinion, successful primary reconstruction combined with multiple secondary revision surgeries could achieve optimal functional and cosmetic results. Further education and emotional support should be emphasized to prevent serious harm.
Mean burn size was similar between OI and CA, but LOS was doubled in the CA group (Table 1). Additionally, the mean operation time was double, and mean revision surgeries were four-fold higher in the CA group despite improvements in operative and medical care. Patients often required more reconstruction procedures for both functional and cosmetic reasons because the face and neck were often involved. For the same reasons, operation times were longer and revision surgeries more numerous. In the OI group, 64% patients were able to return to work and 51% patients were able to return to their pre-injury life. In the CA group, 60% patients were able to return to work; however, only 42% patients were able to return to their pre-injury life. The hand involvement rate was significantly higher in OI patients, most likely because workers did not use protective rubber gloves while working (Table 4).2 Professional training and occupational injury prevention were generally not sufficient for workers handling chemicals. On the contrary, the injury rates to the face, neck, and chest were significantly higher in the CA group, which is similar to the results reported by Branday et al.9 Fifty-one percent to 60% of patients in both groups had successful primary operations and secondary revisions to their hands and were able to return to work. Conversely, even after satisfactory reconstruction and further revisions for face and neck, only 42% of CA patients were able to return to their pre-injury life; the explanation for this seems to be the social stigma attached to such an injury. Therefore, in the authors’ opinion, successful primary reconstruction combined with multiple secondary revision surgeries could achieve optimal functional and cosmetic results. Further education and emotional support should be emphasized to prevent serious harm.  A retro-correlation was seen in terms of patient occupation (Table 2). These data revealed that assault injuries are more common at higher socioeconomic levels, just as occupational injuries are more common among those in the general labor level. Criminal assault injury has been thought to play a distinctive role associated with chemical burns in Taiwan, mainly caused by emotionally out of control lovers, married couples, or common-law marriages. The authors believe that it is a unique phenomenon that happens quite often in Taiwan as a result of a lovers’ quarrel or domestic dispute between people of higher socioeconomic status. The agent used is the most important factor in diagnosing a chemical burn, and successful therapy is dependent upon recognition of the causative agent.5 The severity and potential damage to the affected area depends on type of chemical agent, the amount, the concentration, duration of exposure, and appropriate first-aid management.2,5 Immediate irrigation with a large volume of water will significantly reduce the depth of the injury and shorten hospitalization.13 The primary agents seem to vary with population, geographical location, surrounding industry, and socioeconomic level.2 In Taiwan the major causative agent is sulfuric acid, which accounted for 21.6% of injuries in the OI group and 77.9% in the CA group. The present study compared the number of patients, mean LOS, and mean TBSA. Regarding severity in these two groups, the total burn surface area displayed no obvious differences in a 20-year period. After 2000, in light of advances in burn wound care and surgical techniques, the LOS for occupational injury and assault injury all progressively declined. Assault injury patients with similar TBSA to occupational injury need twice the operative time and have a four-fold increase in revision surgery. This injury involved patients of relatively high socioeconomic status, had a longer LOS, more severe levels of suffering, and is indicative that assault injuries might cause more damage and suffering than occupational injuries, most likely due to the injury location. Head and neck involvement, which usually demanded more delicate debridement, wound care, and revision surgeries, was significantly higher in the CA group. In other words, assault injury patients required more hospitalization time, debridement, and revision surgeries. Therefore, a chemical assault injury is likely to be more dangerous than an occupational chemical injury. Taiwan is a developing country with a growing heavy industrial sector. Initially, the level of education and occupational injury prevention information was much less widespread in the past compared to the present. Efforts to raise awareness of preventing occupational chemical injuries have decreased these injuries greatly in recent years. Labor and civil rights promotion since 2000 has caused the number of injuries and severity of assault injuries to gradually decrease. Heightened concern regarding occupational injury protection, more work-related training duty, public education, and public security have greatly reduced the incidence of these chemical burns.
A retro-correlation was seen in terms of patient occupation (Table 2). These data revealed that assault injuries are more common at higher socioeconomic levels, just as occupational injuries are more common among those in the general labor level. Criminal assault injury has been thought to play a distinctive role associated with chemical burns in Taiwan, mainly caused by emotionally out of control lovers, married couples, or common-law marriages. The authors believe that it is a unique phenomenon that happens quite often in Taiwan as a result of a lovers’ quarrel or domestic dispute between people of higher socioeconomic status. The agent used is the most important factor in diagnosing a chemical burn, and successful therapy is dependent upon recognition of the causative agent.5 The severity and potential damage to the affected area depends on type of chemical agent, the amount, the concentration, duration of exposure, and appropriate first-aid management.2,5 Immediate irrigation with a large volume of water will significantly reduce the depth of the injury and shorten hospitalization.13 The primary agents seem to vary with population, geographical location, surrounding industry, and socioeconomic level.2 In Taiwan the major causative agent is sulfuric acid, which accounted for 21.6% of injuries in the OI group and 77.9% in the CA group. The present study compared the number of patients, mean LOS, and mean TBSA. Regarding severity in these two groups, the total burn surface area displayed no obvious differences in a 20-year period. After 2000, in light of advances in burn wound care and surgical techniques, the LOS for occupational injury and assault injury all progressively declined. Assault injury patients with similar TBSA to occupational injury need twice the operative time and have a four-fold increase in revision surgery. This injury involved patients of relatively high socioeconomic status, had a longer LOS, more severe levels of suffering, and is indicative that assault injuries might cause more damage and suffering than occupational injuries, most likely due to the injury location. Head and neck involvement, which usually demanded more delicate debridement, wound care, and revision surgeries, was significantly higher in the CA group. In other words, assault injury patients required more hospitalization time, debridement, and revision surgeries. Therefore, a chemical assault injury is likely to be more dangerous than an occupational chemical injury. Taiwan is a developing country with a growing heavy industrial sector. Initially, the level of education and occupational injury prevention information was much less widespread in the past compared to the present. Efforts to raise awareness of preventing occupational chemical injuries have decreased these injuries greatly in recent years. Labor and civil rights promotion since 2000 has caused the number of injuries and severity of assault injuries to gradually decrease. Heightened concern regarding occupational injury protection, more work-related training duty, public education, and public security have greatly reduced the incidence of these chemical burns.
Conclusion
A chemical assault burn might cause more damage and suffering than an occupational-related chemical burn. The promotion of occupational injury protection, public empowerment, and public security in recent years has greatly decreased the occurrence and severity of occupational and chemical assault burns. Advances in burn care and surgical procedures have decreased the LOS for these injuries. The intensive and adequate safety education and professional training, protective clothing at the workplace, decreasing criminal assault cases, and establishing more specialized burn centers will further reduce the incidence and severity of chemical burns.
References
1. Barillo DJ, Cancio LC, Goodwin CW. Treatment of white phosphorus and other chemical burn injuries at one burn center over a 51-year period. Burns. 2004;30(5):448–452. 2. Xie Y, Tan Y, Tang S. Epidemiology of 377 patients with chemical burns in Guangdong province. Burns. 2004;30(6):569–572. 3. Curreri PW, Asch MJ, Pruitt BA. The treatment of chemical burns: specialized diagnostic and prognostic considerations. J Trauma. 1970;10(8):634–642. 4. Singer A, Sagi A, Ben Meir P, Rosenberg L. Chemical burns: our 10-year experience. Burns. 1992;18(3):250–252. 5. Li YY, Liu Y. Analysis of 155 patients with chemical injury: a 5-year experience. Burns. 1993;19(6):516–518. 6. Pitkanen J, Al-Qattan MM. Epidemiology of domestic chemical burns in Saudi Arabia. Burns. 2001;27(4):376–378. 7. Purdue GF, Hunt JL. Adult assault as a mechanism of burn injury. Arch Surg. 1990;125(2):268–269. 8. Yeong EK, Chen MT, Mann R, Lin TW, Engrav LH. Facial mutilation after an assault with chemicals: 15 cases and literature review. J Burn Care Rehabil. 1997;18(3):234–237. 9. Branday J, Arscott GD, Smoot EC, Williams GD, Fletcher PR. Chemical burns as assault injuries in Jamaica. Burns. 1996;22(2):154–155. 10. Humphris CJ. Chemical danger. Lancet. 2004;364(9449):1937. 11. Simmons JE. Chemical mixtures: challenge for toxicology and risk assessment. Toxicology. 1995;105(2-3):111–119. 12. Saha A, Kumar S, Vasudevan DM. Factors of occupational injury: a survey in a chemical company. Ind Health. 2008;46(2):152–157. 13. Moran KD, O'Reilly T, Munster AM. Chemical burns. A ten-year experience. Am Surg. 1987;53(11):652–653. Ching-Chun Lin, MD is from the Department of Plastic Surgery, China Medical University Hospital, Taichung, Taiwan and the China Medical University, Taichung, Taiwan; Cho-Kai Wu, MD is from the Department of Internal Medicine, National Taiwan University College of Medicine and Hospital Yun-Lin Branch, Yun-Lin, Taiwan and the Graduate Institute of Clinical Medicine, College of Medicine, National Taiwan University, Taipei, Taiwan; Yi-Fan Wu, MD is from the Department of Community Medicine, Taipei City Hospital, Renai Branch, Taipei, Taiwan; and Jui-Yung Yang, MD and Shiow-Shuh Chuang, MD are from the LinKou Burn Center, Department of Plastic and Reconstructive Surgery, Chang-Gung Memorial Hospital and Chang-Gung University, Taipei, Taiwan. Address correspondence to: Jui-Yung Yang, MD Department of Plastic and Reconstructive Surgery Chang Gung Memorial Hospital 5 Fu-Shin Rd. Gweishan, Taoyuan, Taiwan, 333 Phone: +886-4-22052121 ext. 2020 E-mail: lin.chingchun@gmail.com





