Basal Cell Carcinoma Arising From a Nonhealing Lower Extremity Ulcer: A Case Report
Abstract
Introduction. BCC is a malignancy that arises from the basal cells of the epidermis. Despite being the most common cancer worldwide, it rarely occurs in the setting of long-standing ulceration. Malignant transformation of wounds and scars is typically associated with the development of SCC, as with an MU. Reports in the literature of BCC arising within nonhealing, lower extremity wounds are limited. Case Report. The authors report a case of a 65-year-old man with several comorbidities who presented to the clinic with a nonhealing wound on the right lateral ankle. The wound first began as warts during childhood that had necessitated frequent debridement. The lesions persisted and, 7 years ago, developed into an ulcer with a large fungating mass associated with pain, bleeding, and foul-smelling exudate. Biopsy findings were consistent with infiltrative-type BCC. He was not a surgical candidate given his comorbidities and was instead treated with radiation therapy. No evidence of metastasis was seen on follow-up imaging. Conclusion. This case highlights the importance of prompt biopsy and cultures in patients with suspicious ulcers and wounds that do not respond to appropriate treatment.
Abbreviations
BCC, basal cell carcinoma; IgA, immunoglobulin A; MU, Marjolin ulcer; PG, pyoderma gangrenosum; SCC, squamous cell carcinoma.
Introduction
BCC is a malignancy that arises from the basal cells of the epidermis. It is the most common cancer worldwide, with an incidence of more than 2 million individuals each year in the United States alone.1 The greatest risk factor for developing BCC is exposure to ultraviolet radiation; therefore, sun-exposed areas, particularly of the head and neck, are the most common locations. Despite its prevalence, it rarely arises in the setting of long-standing ulceration.2-6 In this report, the authors present a case of a 65-year-old man found to have a BCC developing in a lower extremity ulcer.
Case Report
A 65-year-old man with a history of hypertension, alcohol use, tobacco use (>50 pack years, quit >15 years prior to presentation), cirrhosis of the liver, and congestive heart failure (ejection fraction of 20%–24%) presented to the clinic for evaluation of a nonhealing ulcer on the right lateral ankle that had persisted for more than 20 years. The wound first began during childhood as warts that necessitated frequent debridement. The lesions persisted and, 7 years previously, developed into an ulcer with a large fungating mass. The mass continued to grow in size and was associated with pain, bleeding with slight abrasion, and a foul odor. Because of constant drainage of a purulent and bloody exudate, the patient self-dressed the ulcer with gauze. He reported that he had never sought any medical care for the ulcer.
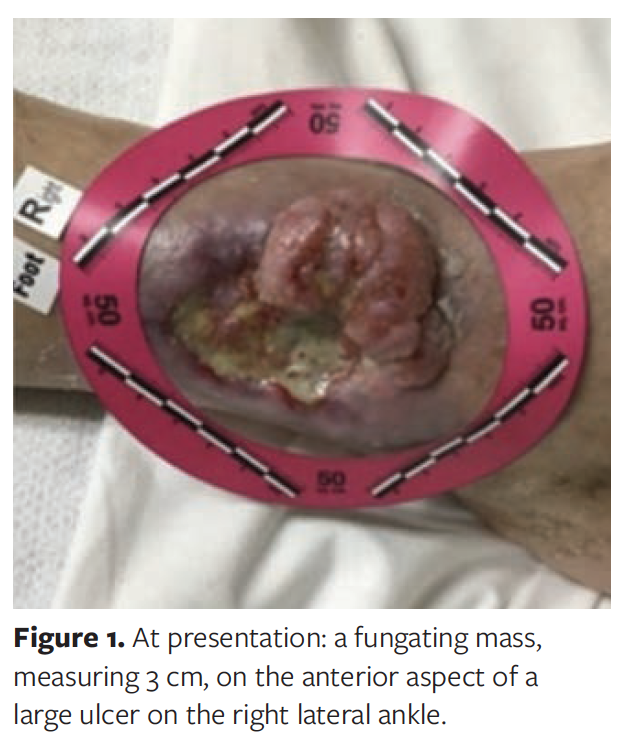
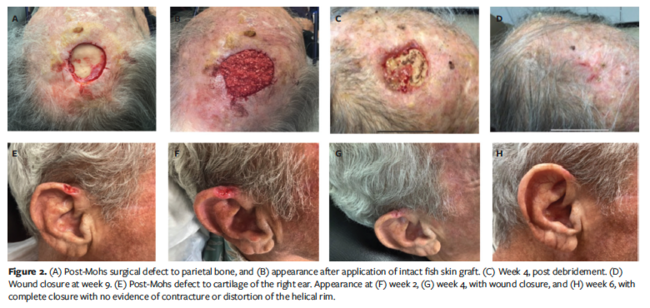
On physical examination, a 3-cm fungating mass was observed on the anterior aspect of an ulcer measuring 8.5 cm × 6.0 cm × 1.0 cm (Figure 1). There were two 4-mm punch biopsies taken from the site. Pathology results were consistent with infiltrative-type BCC, and tissue cultures grew 2+ Proteus mirabilis. The patient was treated with a 10-day course of oral amoxicillin/clavulanate 875 mg every 12 hours. Given the comorbidities, the patient was not a surgical candidate and instead was treated with 6400 cGy of radiation therapy (Figures 2, 3). The patient has remained under surveillance with close follow-up with an oncologist, and no evidence of metastasis has been seen on computed tomography.

Discussion
The transformation of chronic wounds and scars to cutaneous malignancies, termed Marjolin ulcer, was first described in 1828 by the French surgeon, Jean Nicolas Marjolin. Malignancies rarely arise in this setting, but when they do, they are most commonly classified as SCC. In a literature review, 71% of MUs were SCC, 12% were BCC, and 6% were melanomas.5,6 Although the pathophysiology has not been completely understood, it has long been believed that the transformation may occur in part due to chronic irritation and local toxins altering immune mechanisms that protect the skin from neoplastic changes.7 Some common inciting conditions that lead to the development of MUs include burn scars, venous stasis ulcers, osteomyelitis, and pressure ulcers.7 Foreign bodies (which may be mutagenic or tumorigenic) can be a predisposing factor, as was seen in World War II infantrymen who developed BCCs within MUs at the site of grenade fragment wounds.8
A retrospective French study conducted by Combemale et al9 looked at 85 cases of chronic leg ulcers of vascular origin that were complicated by skin cancer. SCC arose in 83 of the 85 cases, whereas BCC only arose in 2 of the 85 cases. Another prospective study of 154 cases of chronic leg ulcers revealed skin cancer in 16 of the ulcers. Of the 16 cases, 9 were SCC, 5 were BCC, 1 was melanoma, and 1 was a leiomyosarcoma.10 Studies have demonstrated that, although the absolute risk is rare, SCC can develop as a direct complication of these chronic leg ulcers.11
Current literature suggests that BCCs can arise from venous stasis ulcers 1.5% to 15% of the time.12 In the case of the authors’ patient, without previous histological examination, it is unclear whether he had a malignant transformation of a prior longstanding ulcer or if the BCC was a primary neoplasm disguised as a potential vascular ulcer. Nonetheless, the development of BCC is relatively uncommon in such settings. Morphologically, the cancer tends to have the appearance of healthy granulation tissue with an exuberant, translucent appearance that extends beyond the ulcer’s margins.13 BCCs have also been reported in cleft lip repair and other surgical scars, as well as in keloid scars.14-16
In addition to malignancies, other diagnoses to consider in the case of a fungating mass developing within a long-standing ulcer include various infections, such as mycobacterial infection, syphilis, histoplasmosis, coccidioidomycosis, blastomycosis, and leishmaniasis, especially in cases where the host is immunocompromised. Any ulcer that has been chronically worsening or present for an extended period of time without healing, has been prone to bleeding, or has not been responding to appropriate treatment should promptly undergo a biopsy.
As patients with BCC have a 10-fold increased risk of developing BCC at distant sites, the implications of a missed diagnosis are severe; some authors recommend serial biopsies every 3 to 6 months in the aforementioned situations.12 It is also important to culture the site to assess for any infectious organisms that may be contributing to the ulceration when clinical signs are present. PG is also an important consideration for lower extremity lesions presenting with a rolled, undermined, violaceous border. However, it is a diagnosis of exclusion and can be considered after malignancy, vasculitis, and infection have been ruled out if biopsy results are consistent with PG (diffuse dermal neutrophilic infiltrate) and if the patient has risk factors (eg, inflammatory bowel disease, IgA monoclonal gammopathy, hematologic malignancies).17
Surgical resection is the treatment of choice for localized BCCs, whether through wide local excision or Mohs micrographic surgery. Nonsurgical options (particularly as adjuvant therapy in metastatic cases) include Hedgehog pathway inhibitors, such as vismodegib and imiquimod; radiotherapy; electrodesiccation and curettage; chemotherapy, such as 5-fluorouracil; photodynamic therapy; and cryotherapy.18 For fungating and ulcerating wounds, optimal wound care is of utmost importance; negative pressure wound therapy devices, among others, may be useful.
Limitations
The current case is limited by the scarce reports of patients with BCC in a long-standing lower extremity wound. Although this case report only includes a single patient, it highlights the importance of prompt biopsy in patients with suspicious wounds that do not respond appropriately to treatment. Another important limitation of this case is that there was no record of a prior biopsy performed on the wound. Therefore, it is unclear whether the patient had a malignant transformation of a prior long-standing ulcer or if the BCC was a primary neoplasm disguised as a potential vascular ulcer.
Conclusion
While the development of skin cancer within wounds is rare, there are cases describing the development of SCC as a direct complication of chronic leg ulcers. The reports of BCC arising in such a setting are notably more limited. This case report describes the diagnosis and treatment of BCC in a 65-year-old man presenting with a large fungating mass developing within an ulceration. Patients with similar long-standing wounds that are not responding to appropriate treatment may benefit from having a biopsy performed to rule out malignancy and to guide further treatment.
Acknowledgments
Authors: Sidra Deen, BS; Usman Asad, MD; and Edward Lee Poythress, MD
Affiliations: Baylor College of Medicine, Houston, TX
Disclosure: The authors disclose no financial or other conflicts of interest.
Correspondence: Edward Lee Poythress, MD; One Baylor Plaza, Room M210 MS: BCM368, Houston, TX 77030; edwardp@bcm.edu
References
1. Marks J, Miller J. Epidermal Growths. In: Lookingbill and Marks’ Principles of Dermatology. 6th ed. Elsevier; 2019:41-61.
2. Pekarek B, Buck S, Osher L. A comprehensive review on Marjolin’s ulcers: diagnosis and treatment. J Am Col Certif Wound Spec. 2011;3(3):60-64. doi:10.1016/j.jcws.2012.04.001
3. Schwarze HP, Loche F, Gorguet MC, Kuchta J, Bazex J. Basal cell carcinoma associated with chronic venous leg ulcer. Int J Dermatol. 2000;39(1):78-79. doi:10.1046/j.1365-4362.2000.00855.x
4. Blank AA, Schnyder UW. Squamous cell carcinoma and basal cell carcinoma within the clinical picture of a chronic venous insufficiency in the third stage. Dermatologica. 1990;181(3):248-250. doi:10.1159/000247946
5. Day DL, Chakari W, Matzen SH. Malignant transformation of a non-healing traumatic wound on the lower extremity: a case report. Int J Surg Case Rep. 2018;53:468-470. doi:10.1016/j.ijscr.2018.11.026
6. Kowal-Vern A, Criswell BK. Burn scar neoplasms: a literature review and statistical analysis. Burns. 2005;31(4):403-413. doi:10.1016/j.burns.2005.02.015
7. Shah M, Crane JS. Marjolin Ulcer. In: StatPearls. StatPearls Publishing; May 8, 2022.
8. Rieger UM, Kalbermatten DF, Wettstein R, Heider I, Haug M, Pierer G. Marjolin’s ulcer revisited – basal cell carcinoma arising from grenade fragments? Case report and review of the literature. J Plast Reconstr Aesthet Surg. 2008;61(1):65-70. doi:10.1016/j.bjps.2006.05.018
9. Combemale P, Bousquet M, Kanitakis J, Bernard P; Angiodermatology Group, French Society of Dermatology. Malignant transformation of leg ulcers: a retrospective study of 85 cases. J Eur Acad Dermatol Venereol. 2007;21(7):935-941. doi:10.1111/j.1468-3083.2006.02118.x
10. Senet P, Combemale P, Debure C, et al. Malignancy and chronic leg ulcers: the value of systematic wound biopsies: a prospective, multicenter, cross-sectional study. Arch Dermatol. 2012;148(6):704-708. doi:10.1001/archdermatol.2011.3362
11. Baldursson B, Sigurgeirsson B, Lindelöf B. Venous leg ulcers and squamous cell carcinoma: a large-scale epidemiological study. Br J Dermatol. 1995;133(4):571-574. doi:10.1111/j.1365-2133.1995.tb02707.x
12. Nicoara M, Bain K, Patel R, Jaikaran O, Hingorani A, Asher E. Malignant transformation of nonhealing ulcer—basal cell carcinoma. Ann Vasc Surg. 2021;70:565.e7-565.e10. doi:10.1016/j.avsg.2020.01.100
13. Harris B, Eaglstein WH, Falanga V. Basal cell carcinoma arising in venous ulcers and mimicking granulation tissue. J Dermatol Surg Oncol. 1993;19(2):150-152. doi:10.1111/j.1524-4725.1993.tb03445.x
14. Wright MW, McCarthy RA, Kelly EB, Wright ST, Wagner RF. Basal cell carcinoma arising in a cleft lip repair scar. Dermatol Surg. 2001;27(2):195-197. doi:10.1046/j.1524-4725.2001.00181.x
15. Ozyazgan I, Kontaçs O. Basal cell carcinoma arising from surgical scars: a case and review of the literature. Dermatol Surg. 1999;25(12):965-968. doi:10.1046/j.1524-4725.1999.99192.x
16. Goder M, Kornhaber R, Bordoni D, Winkler E, Haik J, Tessone A. Cutaneous basal cell carcinoma arising within a keloid scar: a case report. Onco Targets Ther. 2016;9:4793-4796. doi:10.2147/OTT.S113724
17. Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. Elsevier; 2017.
18. Basset-Seguin N, Herms F. Update in the management of basal cell carcinoma. Acta Derm Venereol. 2020;100(11):adv00140. doi:10.2340/00015555-3495