



Evaluating the Number of Cellular and/or Tissue-Based Product Applications Required to Treat Diabetic Foot Ulcers and Venous Leg Ulcers in Non-Hospital Outpatient Department Settings
Abstract
Background. There is substantial literature supporting the use of cellular and/or tissue-based product (CTP) in managing Wagner grade 1 and 2 diabetic foot ulcers (DFUs) and, to a lesser extent, venous leg ulcers (VLUs). Several studies advocate CTP therapy as an effective method for promoting healing in chronic DFUs and VLUs. Objective. To evaluate how the number of CTP applications affect healing and wound area reduction (WAR) rates of DFUs and VLUs. Methods. A multicenter private wound care practice, electronic health record, and database were used to analyze Medicare patients receiving CTPs between January 1, 2018, and December 31, 2023. Wound treatments occurred in the nursing home, private office, and home settings, not in hospital outpatient department settings. This privately funded, non–vendor-sponsored, real-world retrospective analysis included wound closure and WAR rates after each CTP application. Analysis includes current (2024) aspects of proposed local coverage determination changes that limit the number of CTP applications to 4. A paired t test was used to compare mean wound area before CTP applications and after completing CTP applications over a 16-week period. Effect sizes were analyzed using Cohen d, and correlations between the number of CTP applications and WAR were determined using the Pearson correlation coefficient. Results. A total of 257 wounds were reviewed for analysis, of which 123 were DFUs and 134 were VLUs. For both DFUs and VLUs, there was a significant difference in the average initial wound areas (cm2) compared with the average wound areas after the CTP application series (P < .001). Conclusion. This comprehensive retrospective real-world analysis of Medicare patients receiving CTP therapy in conjunction with standard of care treatment of DFUs and VLUs demonstrated significant reduction in the average wound area after completing a CTP application series. The results of this study could be used as a guide for the average number of CTP applications required for the effective treatment of DFUs and VLUs.
Abbreviations: AR, accounts receivable; CI, confidence interval; CTP, cellular and/or tissue-based product; DFU, diabetic foot ulcer; EHR, electronic health record; Hb, hemoglobin; HOPD, hospital outpatient department; ICD-10, International Statistical Classification of Diseases and Related Health Problems, Tenth Revision; LCD, local coverage determination; MAC, Medicare Administrative Contractor; SD, standard deviation; SOC, standard of care; VLU, venous leg ulcer; WAR, wound area reduction.
Introduction
Recent epidemiological data indicate an estimated 6.3% prevalence of DFU among persons with diabetes in the United States.¹ In addition, there is a concerning rise of up to 50% in overall amputation cases across various regions of the United States since 2009, particularly among young individuals and racial and ethnic minority groups, marking a reversal from previous declines.1
Despite ongoing efforts to enhance DFU care, amputation rates have not decreased.2-5 Moreover, evidence suggests widening disparities in DFU care, raising concerns about equity in diabetes care.2-5
Similarly, studies have reported a prevalence rate of 0.32% and an incidence rate of 0.17% for VLUs among US patients with venous insufficiency.6 VLUs remain a significant concern globally. Despite adequate care, up to 20% of VLUs do not heal within 2 years, especially in the lower extremties.6-8 Prevalence rates underscore the associated complications of these chronic wounds and their substantial public health effect on the US economy.9 An urgent need exists to identify effective medical strategies to ensure prevention and management of DFU and VLU.
Despite advancements in health care, chronic nonhealing wounds impair patients’ quality of life, prolong suffering, and impose a substantial economic burden on patients. In recent years, interest has grown in the use of innovative strategies for managing DFUs and VLUs including CTPs and cellular, acellular, and matrix-like products. Over the past 2 decades, CTPs have emerged as promising therapeutic options to facilitate wound closure and promote tissue regeneration.10 However, understanding the optimal number of CTP applications required to effectively reduce wound size remains a critical and understudied aspect of wound care.
The goal of the current study is to present real-world evidence to address this knowledge gap by investigating the relationship between the number of CTP applications and wound size reduction in DFUs and VLUs. By identifying the ideal number of CTP applications needed to reduce wound area effectively and promote healthy tissue regeneration, the authors of the current study aim to enhance clinical outcomes, improve patient care, and contribute to advancing wound management strategies.
Background
There is sufficient literature to support the use of cellular and acellular CTPs in the management of Wagner grade 1 and 2 DFUs and, to a lesser degree, in the management of VLUs. Several studies have emerged and have advocated for the use of CTP therapy as an effective means of promoting wound healing in chronic wounds.11,12 Cellular and acellular CTPs are used to promote wound closure through tissue regeneration and facilitation of repair through extracellular remodeling. Advances in tissue engineering of CTPs have provided scaffolds and growth factors to accelerate chronic wound healing.11,12 Studies have shown that placental-based CTPs, such as amniotic membrane allografts, reduce healing time in chronic DFUs compared with conventional wound healing methods.6,13-17 Similarly, several studies have shown that dehydrated human amnion/chorion allografts, in addition to SOC treatment, significantly improved healing compared with SOC alone.18 The evidence regarding the efficacy of CTPs in the management of chronic wounds is sound. However, there is a gap in the literature concerning the effect of application of CTP treatment on wound closure rates and the number of CTP applications needed to sufficiently reduce wound size.
Governing medical agencies play a crucial role in approving the number and type of CTP applications for managing DFUs and VLUs. These regulatory bodies comprehensively have different roles: to evaluate the safety and efficacy of CTP applications, strengthen and modernize the US health care system, provide access to high-quality care, and improve health at lower cost. Although the evidence supports the efficacy of CTP applications to enhance the number of healed Wagner grade 1 and 2 DFUs and VLUs and to decrease time to closure, more research is needed to determine the number of CTP applications needed to achieve complete healing of DFUs and VLUs. In addition, there is a need for more research on amputation prevention and enhanced quality of life. As of May 2024, a proposed LCD limits the number of CTP applications to 4 in a 12-week period.19 The current study aims to determine the number of CTP applications necessary to achieve optimal WAR and closure rates of DFUs and VLUs. It should be noted that the current study was undertaken prior to publication of the proposed LCD.
Methods
Data source and definitions
The database and patient EHRs of a private wound practice with multiple offices in rural Louisiana and Mississippi were searched for all patients with Medicare insurance who received CTP applications between January 1, 2018, and December 31, 2023. Wound treatment occurred in non-HOPD settings, including outpatient clinics, nursing home facilities, and patients’ homes. AR reports were run for ICD-10 diagnosis codes to identify patients with DFU and VLU. Wound etiologies were further investigated using AR reports documented within the EHR. Lastly, an AR report was completed to identify patients who received CTP applications between January 1, 2018 and December 31, 2023, and to identify wound size at each CTP application. All demographic data and wound characteristics were obtained through manual review of each chart.
All patients receiving CTP applications initially received SOC for at least 4 weeks. Patients with less than 50% WAR despite 4 weeks of SOC qualified to receive a CTP. A CTP application series was defined as less than or equal to 10 CTPs within 16 weeks in a single patient. These patients also met the LCD, set forth by the MAC, for DFU and VLU criteria to qualify for CTP treatment. Patients who received fewer than 10 CTP applications were included for analysis if the wound healed prior to completing a 10 CTP application series.
A DFU was defined as a wound located on the ankle or foot in a patient with a diagnosis of diabetes. A VLU was defined as a wound on the lower extremity in a patient diagnosed with venous insufficiency. Initial wound measurement was defined as the wound size (area) at the first CTP application. The last wound measurement was defined as the wound size at the last CTP application or 1 week after the last CTP application. Healed wounds were defined as having a 99% to 100% WAR rate due to EHR documentation requirements to classify wounds as healed. Healed percentage parameters were necessary to establish because wound providers (physicians, nurse practitioners, physician assistants) would occasionally document healed wounds as 0.01 cm² to ensure measurements and pictures remained accessible for continued patient follow-up. Patients continued follow-up per provider discretion to ensure maintenance of wound closure until they were discharged from wound medicine services; at that time the healed wound would be documented as 0.0 cm2.
Design and procedures
This retrospective study identified Medicare patients who had received CTP treatment for DFUs and VLUs. The main objective was to evaluate the number of CTP applications required to achieve wound closure and WAR rates of DFUs and VLUs. This study was privately funded, and no vendor sponsorship or grants were accepted. These CTPs were reimbursed per the local MAC during the duration of the study. Institutional review board approval was obtained for this retrospective study.
Wound providers completed CTP applications per wound practice policy. This policy ensured that all wounds underwent a thorough 4-week SOC treatment process, including sharp and/or ultrasonic debridement, before a CTP was placed onto the wound bed. Wound medicine providers also ensured that the wound was free of any necrotic tissue or infection and that optimal perfusion and sufficient offloading or compression parameters were in place prior to beginning the CTP application series. Smoking cessation counseling was done when applicable. Uncontrolled diabetes was addressed through diabetes diet counseling, medication adjustment and compliance encouragement, and referral to a primary care physician and/or endocrinologist when needed. Primary dressings were placed to ensure CTP applications were anchored, and secondary dressings were placed to ensure drainage control of wounds. Offloading was accomplished by total contact cast placement, and ambulatory venous pressure reduction was accomplished by compression therapy. These therapies were performed at the provider’s discretion and were individualized to each patient. Secondary dressings were changed 2 or 3 times weekly, depending on wound drainage. Primary dressings stayed in place for approximately 7 days. Patients followed up with the wound provider weekly for repeat CTP application until either the wound healed or all 10 CTP applications had been completed. No patients received more than 10 CTP applications due to the LCD policy limitations set forth by the MAC.
Outcome measures
Primary outcome measures included the percentage WAR at the time of each CTP application and comparison of WAR from initiation to completion of the CTP application series. Secondary outcomes included average wound size at each CTP application and the number of healed wounds after completing the CTP application series. Patient demographics were reported for descriptive purposes of the sample studied. Comorbidity selection was determined after a manual chart review of common comorbidities seen in the private wound practice. The mean (SD) HbA1c level was also included to identify patients with diabetes. Wound characteristics included initial wound depth prior to CTP application. CTPs were reported to describe the nature of the CTP used.
Sample selection
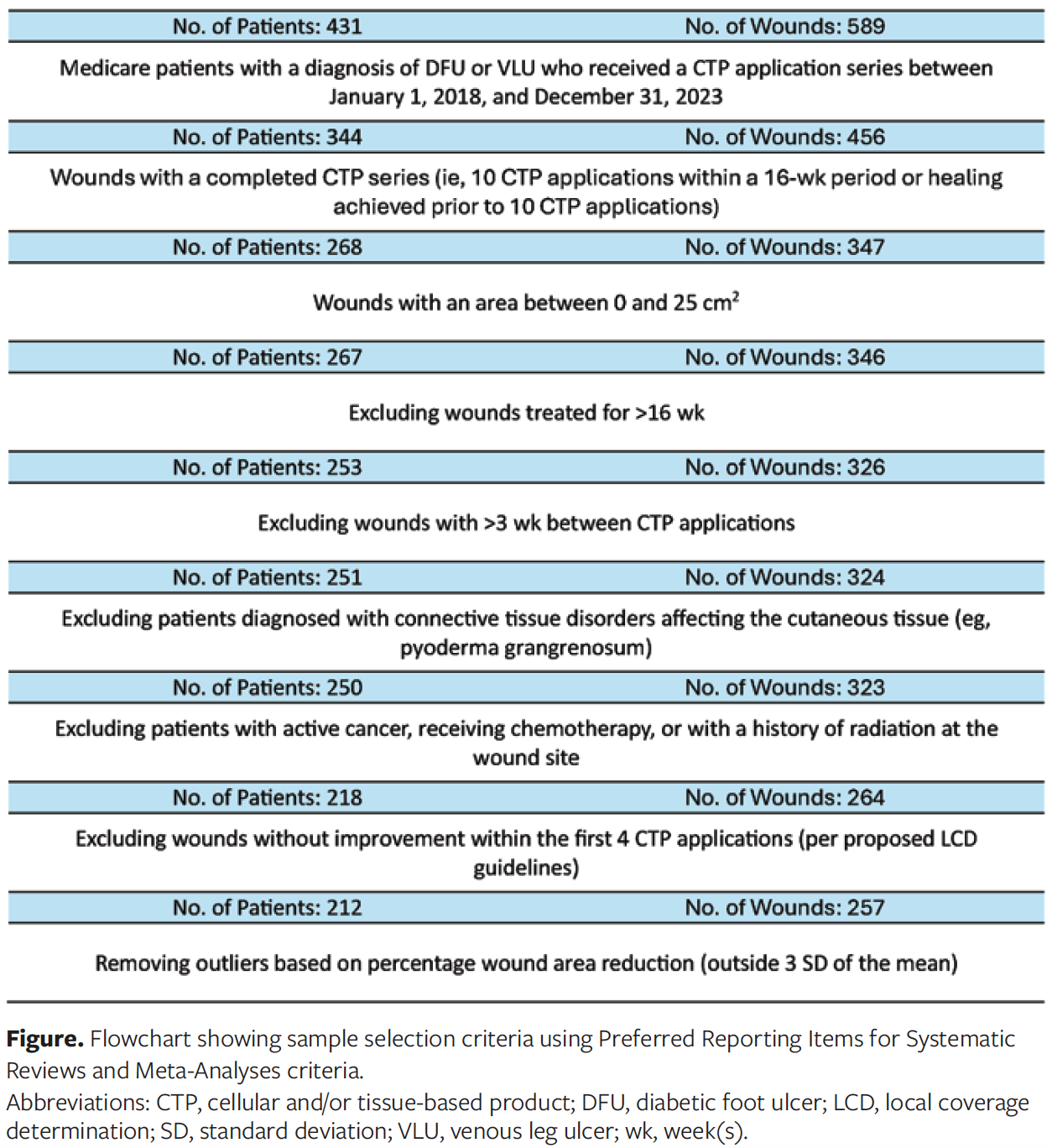
A data set was generated after first identifying patients with Medicare insurance who had received a CTP application between the eligibility period of January 1, 2018, and December 31, 2023. Medicare remained the primary inclusion criterion, given that most patients receiving CTP therapy were approved for 10 CTP applications and could complete the proposed study intentions. ICD-10 diagnosis codes were also used to identify patients with DFUs and VLUs. Wound area between 0 cm² and 25 cm² was set for the sample of interest for consistency with most prior CTP studies in the literature.4,12,13,20,21
Patients who had received more than 10 CTP applications or who did not complete their CTP application series within 16 weeks were excluded from the study to ensure the standardization of CTP series treatment for DFUs and VLUs. Patients with more than 21 days between CTP applications were also excluded from review. Patients undergoing CTP applications whose wounds continually increased in size after the fourth CTP application were also excluded from the study. This criterion was established per the current proposed LCD policy guidelines at the time of data retrieval (May 5, 2024), which indicated that repeat CTP applications should not be continued when previous applications are “unsuccessful,” that is, variables exist that prevent progression to wound closure, including an increase in wound size, and no signs or indications of wound improvement are present.19 Patients with a diagnosis of connective tissue disease were evaluated to determine if the connective tissue disease affected the cutaneous tissue (eg, Raynaud disease, calciphylaxis, pyoderma gangrenosum). Patients with connective tissue diseases affecting the cutaneous tissue were excluded. Patients receiving chemotherapy or radiation at the time of CTP application or who had previously received radiation at the site of the wound being treated were excluded, given the effects of radiation and resulting impaired cellular activity. Additional exclusion criteria are listed in the Figure.
Analysis
Descriptive data included percentage WAR, which was computed by obtaining manual wound measurements prior to each CTP application and 1 week following the completion of the CTP application series.
Descriptive analysis was conducted using Microsoft Excel (Microsoft Corporation) for patient demographics and baseline characteristics of patients and wounds. Descriptive statistics were also conducted for average wound size after each CTP application, average number of CTP applications, and percentage WAR after each CTP application. Additionally, the average values of characteristics such as HbA1c level, CTP used, and race or ethnicity of patients whose wounds were noted to have healed were also reported. By setting limits on the number of CTP applications, minority populations may be disproportionately affected. These minority communities often face higher rates of chronic wounds and limited access to health care services, meaning that restrictive policies could exacerbate existing health disparities. Understanding these disparities helps in tailoring treatment strategies. Ensuring diverse representation in research studies helps in generalizing findings across populations. It ensures that the benefits of research are equitable and applicable to all racial and ethnic groups. By assessing race and ethnicity, researchers can aim to develop a comprehensive understanding of the multifaceted influences on DFUs and VLUs, leading to more effective and inclusive health care solutions. Race and ethnicity were self-reported.
Inferential data included analyses to compare the initial wound area before the CTP application series began and the last wound area after the completion of a CTP series. Inferential analysis was conducted using SPSS version 29.0.1.0 (IBM Corporation) for DFUs and VLUs. A paired t test was used to compare mean wound area before and after the CTP application series. Effect sizes were determined using Cohen d. Correlations between wound sizes and the number of CTP applications were determined using the Pearson correlation coefficient. A 95% CI was used, with alpha set at .05 as the level of significance. Outliers were removed using z scores to determine percentage WAR falling outside 3 SDs of the mean.
Patient, wound, and product characteristics
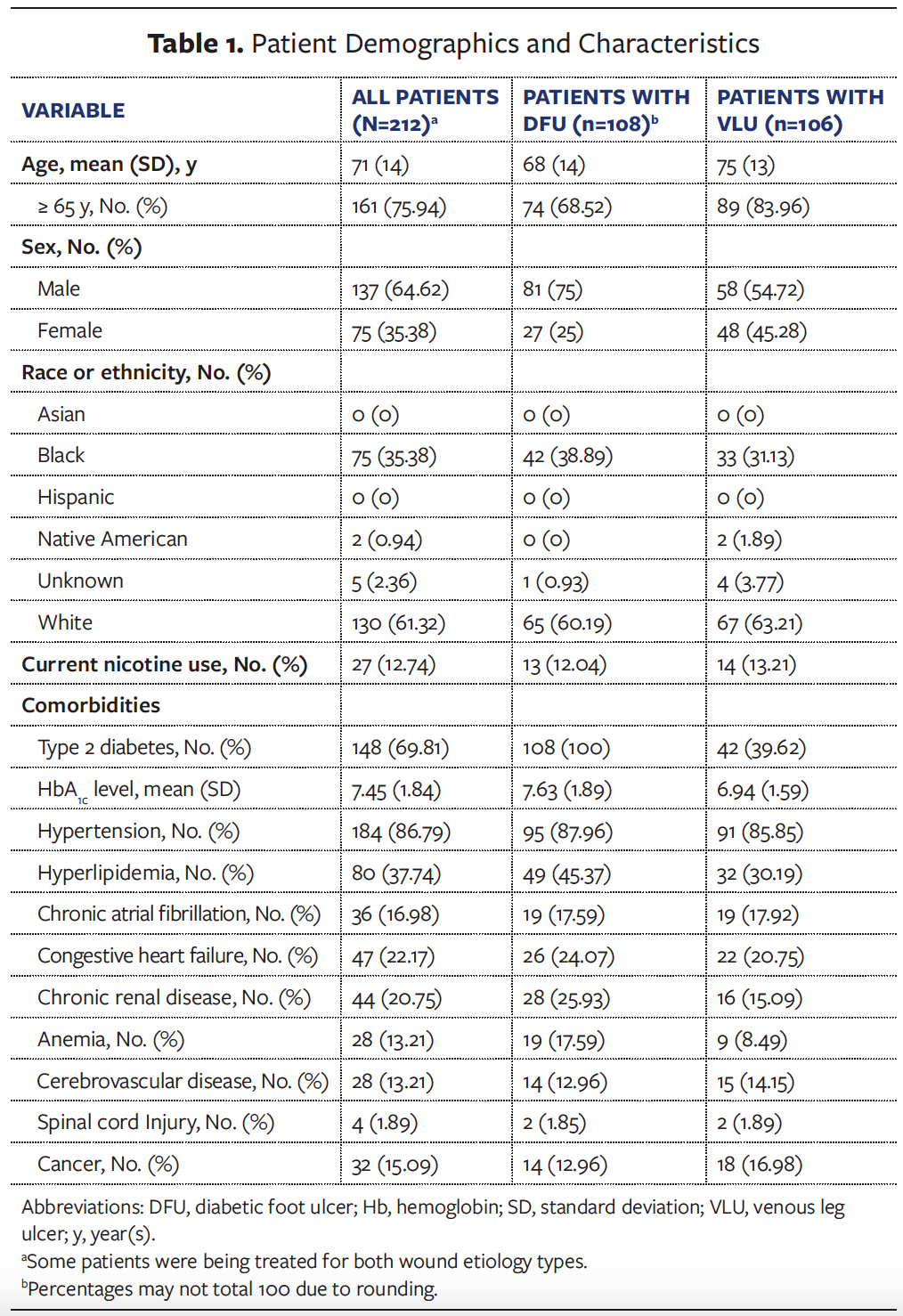
Patient demographics are noted in Table 1. Overall, the majority of the sample chosen for retrospective review was male (64.62%), and 75.94% of the sample was aged 65 years or older. Most patients were Black (35.38%) or White (61.32%), and 12.74% were current nicotine users. Diabetes and hypertension were the leading comorbidities in the reviewed sample.
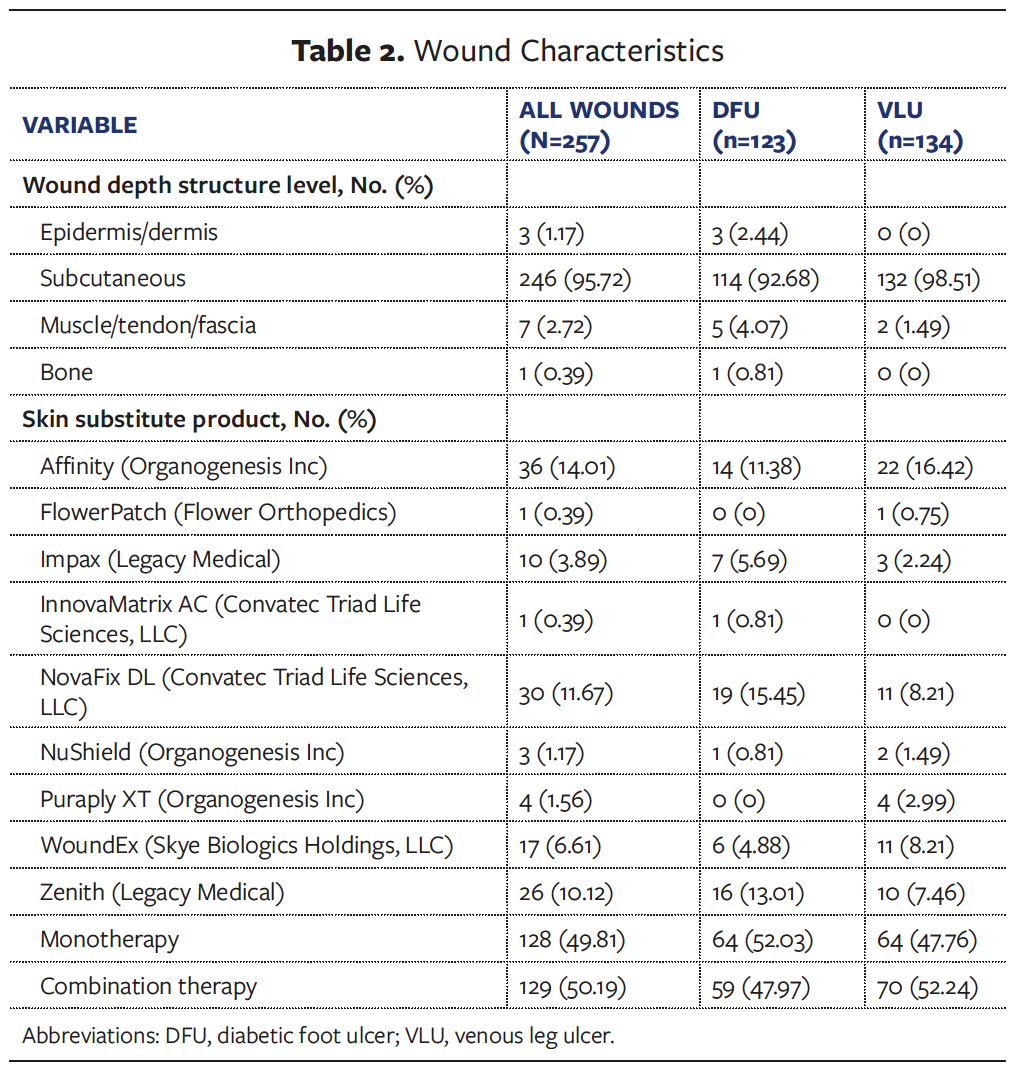
Wound characteristics are listed in Table 2. The majority of wounds reviewed for the retrospective study had a depth to the subcutaneous tissue level, that is, they were full-thickness wounds (95.72%). CTP application for treatment consisted of either monotherapy (49.81%) or combination therapy (50.19%).
Results
A total of 257 wounds were reviewed for analysis, of which 123 were DFUs and 134 were VLUs. The average wound area decreased with each CTP application for both DFUs and VLUs, as seen in Table 3.
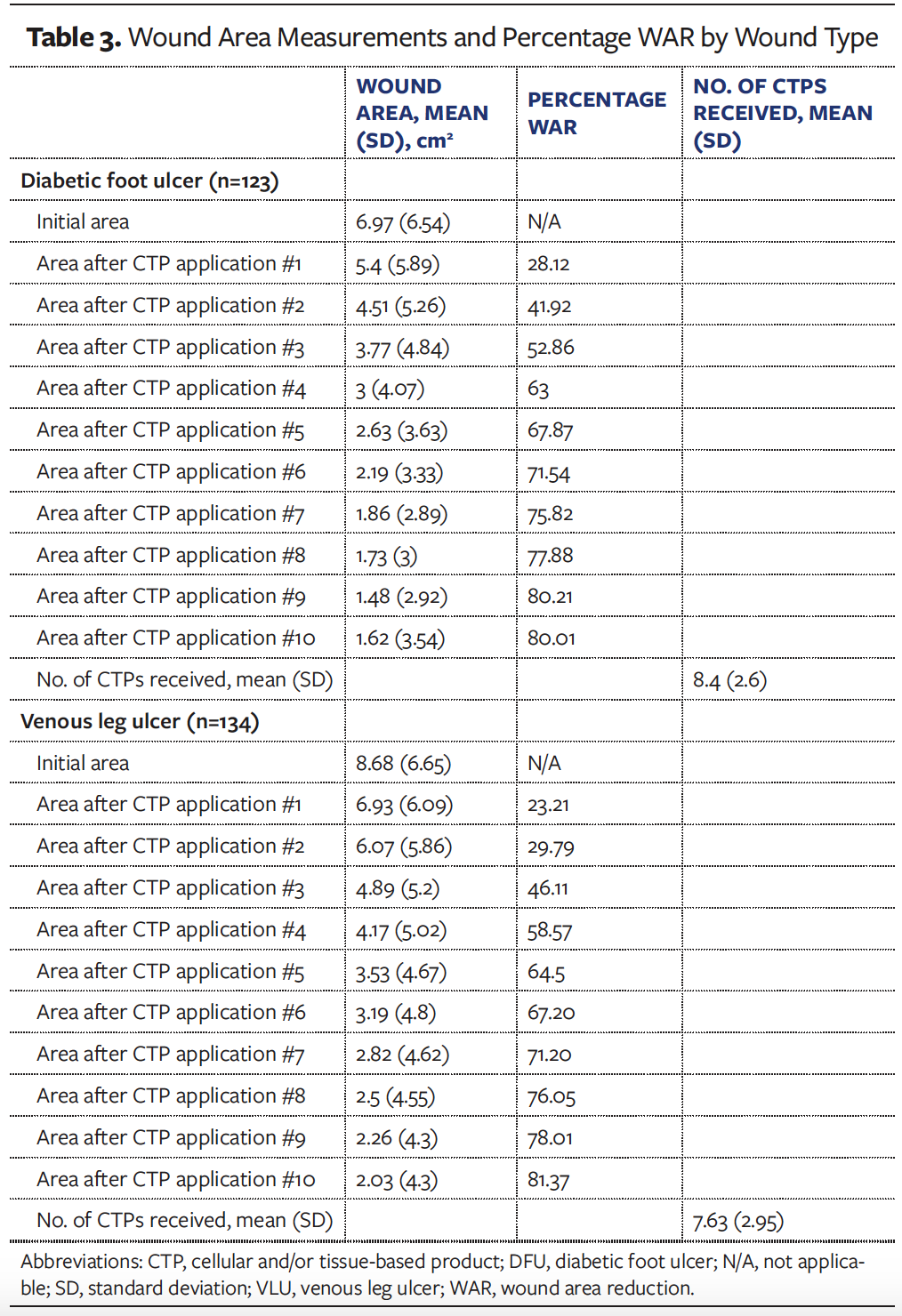
In the DFU sample, the mean (SD) initial wound area was 6.97 (6.54) cm2, and the mean (SD) wound area after the last CTP application was 1.62 (3.54) cm2. The average percentage WAR was also noted to increase with each application. In the DFU sample, the mean (SD) number of CTP applications was 8.4 (2.6). Similar average values were noted with VLUs throughout CTP treatment. In the VLU sample, the mean (SD) initial wound area was 8.68 (6.65) cm2, and the mean (SD) wound area after the last CTP application was 2.03 (4.3) cm2. The mean (SD) number of CTP applications was 7.63 (2.95). The average percentage WAR was also noted to increase with each application.
Wound size and number of CTP applications
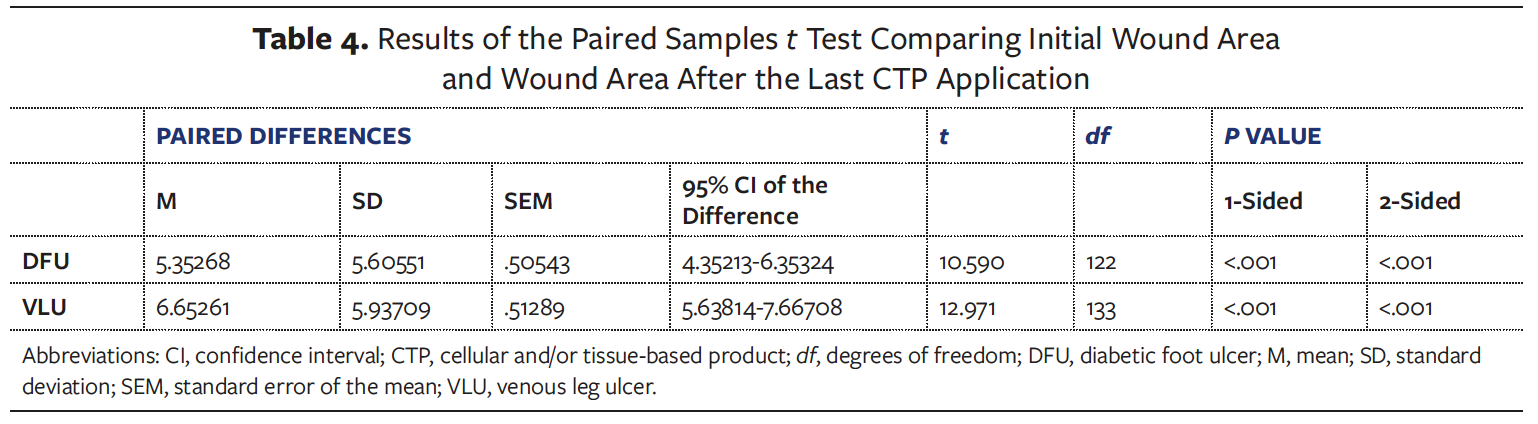
A paired t test was used for DFUs and VLUs to determine whether there was a clinically significant difference between initial wound area and final wound area after a CTP application series. The results of the analysis revealed a significant decrease in mean (SD) DFU area after completion of the CTP series compared with initial DFU area (1.62 [3.54] cm2 vs 6.97 [6.54] cm2; t(122) = 10.59; P < .001). As measured by Cohen d, the effect size was 0.96, indicating a large effect before and after CTP application in the management of DFU. Similar results were observed with VLU area, with a significant decrease in mean (SD) wound area after completion of the CTP series compared with initial wound area (2.03 [4.3] cm2 vs 8.68 [6.65] cm2, t(133) = 12.97; P < .001). Cohen d analysis showed an effect size of 1.1, indicating a large effect before and after CTP application for VLU treatment. Results of the paired t test are shown in Table 4.
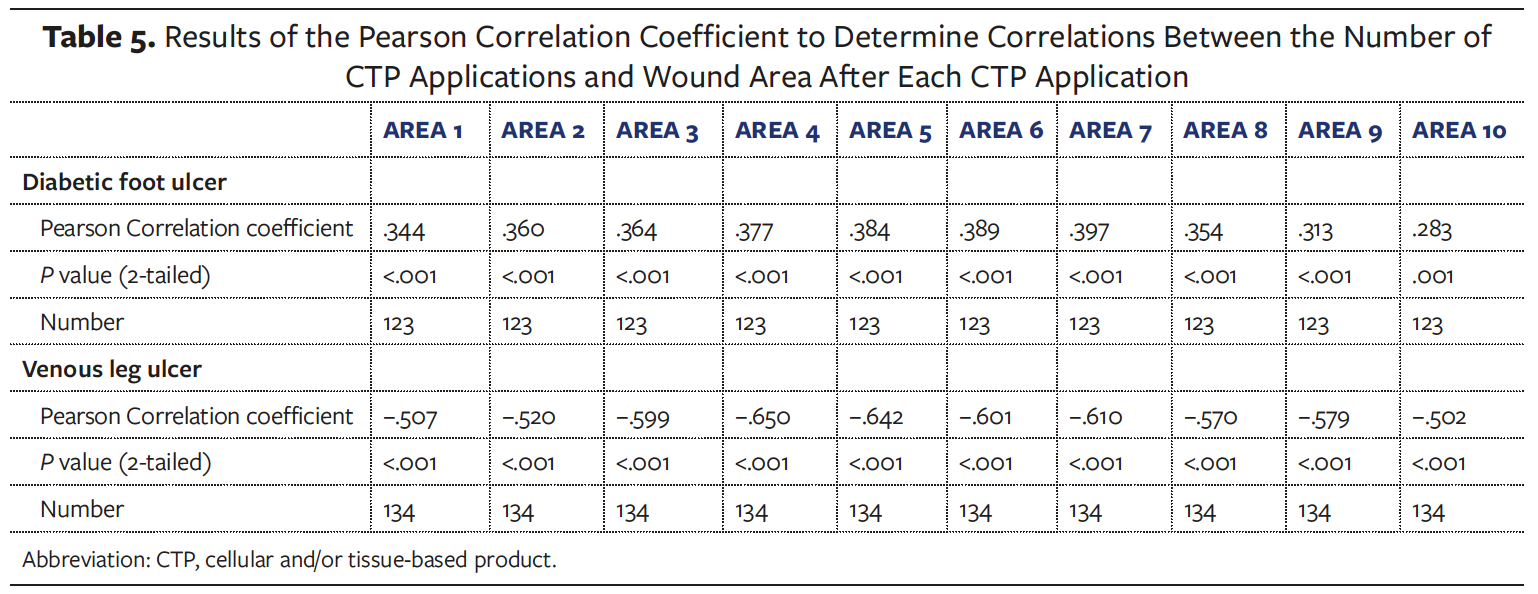
The Pearson correlation coefficient was used to determine correlations between wound area after each CTP application and the number of CTP applications in the series (Table 5). For the DFUs, wound area after each CTP application was found to have a weak positive correlation with the number of CTP applications, with the area after the first CTP application exhibiting a correlation of r(123) = .34 (P < .001) and after the 10th CTP application exhibiting a correlation of r(123) = .28 (P = .001). However, among the VLUs treated with CTP applications, wound area after each CTP application was found to have a moderate negative correlation in relation to the number of CTP applications, with the area after the first CTP application exhibiting a correlation of r(134) = .51 (P < .001), and after the 10th CTP application exhibiting a correlation r(134) = −.50 (P < .001).
Healed wound characteristics
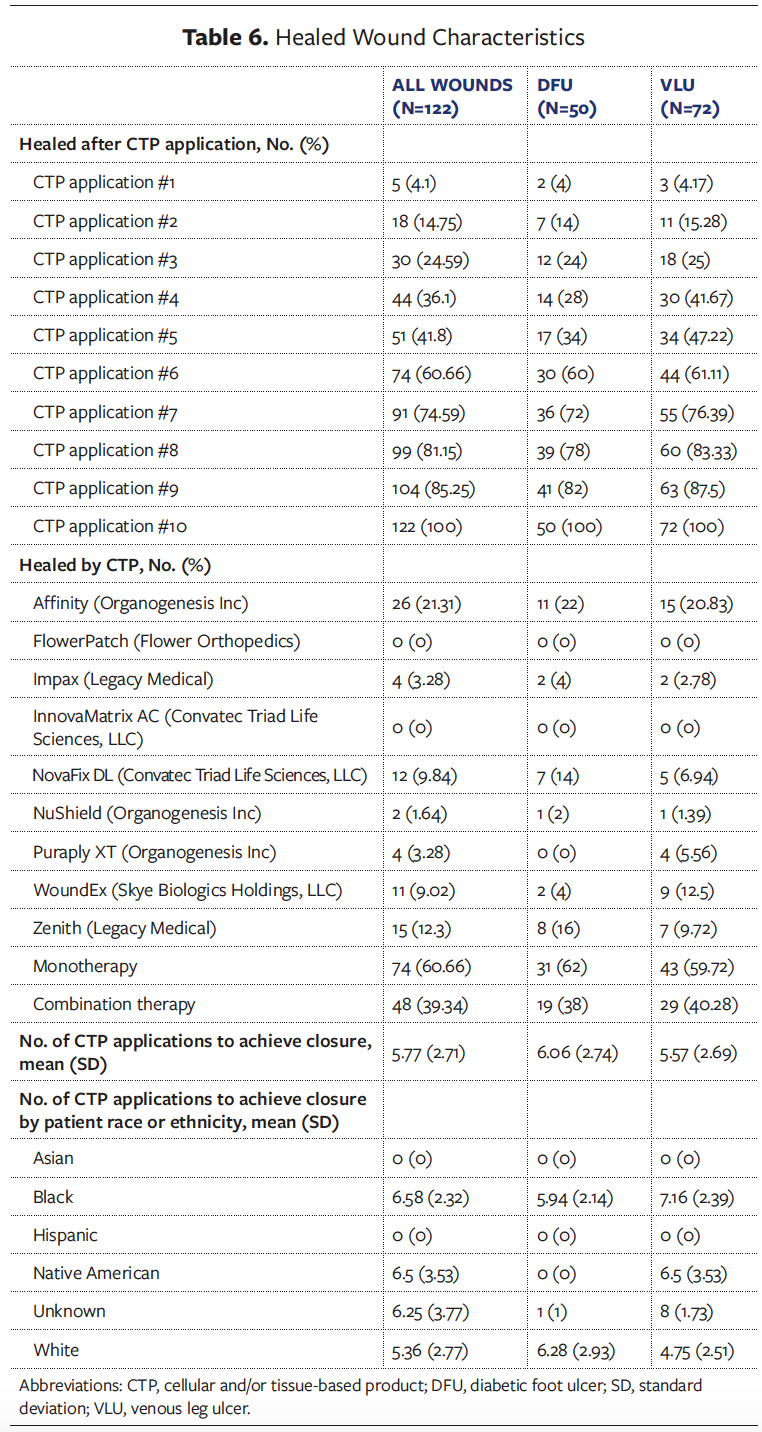
Of the 257 wounds in the study, 122 healed within a 10 CTP application series (47.47%). Of these 122 wounds, 50 (40.98) were DFUs and 72 (59.02) were VLUs. The CTPs used varied, with 74 (60.66%) of the healed wounds receiving monotherapy CTP applications and 48 (39.34) receiving a combination of several CTPs throughout the CTP series.
The average number of CTP applications to achieve wound closure varied by race, with Black patients receiving a higher mean (SD) of 6.58 (2.32) CTP applications, compared with 6.5 (3.53) for Native American patients and 5.36 (2.77) for White patients (Table 6).
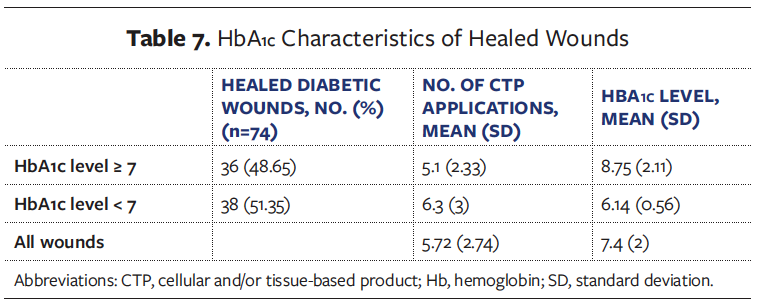
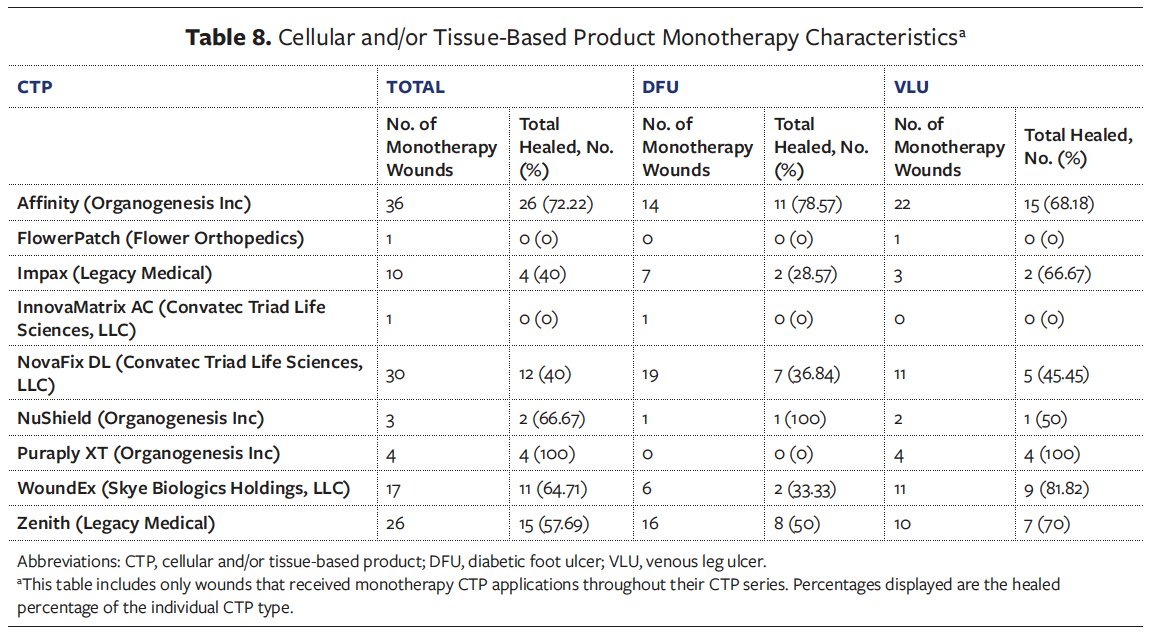
The mean (SD) HbA1c level for all healed wounds was 7.4 (2) (Table 7). CTP monotherapy characteristics were also reviewed during the analysis and are shown in Table 8. All wounds with monotherapy CTP types varied in total number healed.
Discussion
The current study evaluated 2 clinically relevant end points: the incidence of complete wound closure and WAR rates during CTP treatment. Primarily, the focus was on determining the necessary number of CTP applications for adequate wound reduction and closure.
SOC treatment for DFUs and VLUs includes sufficient debridement, offloading, compression, drainage control, and treatment of infection, as well as optimization of blood glucose, nutrition, and circulation. Conventional therapy remains the primary approach for managing DFUs and VLUs. CTP therapy should not be viewed as a standalone treatment option but rather an adjunct to SOC treatment.
Average WAR was noted after each CTP application. The most considerable percentage WAR was noted with the first 7 CTP applications after which rates began to plateau. Further, significant correlations were noted regarding the number of CTP applications and WAR in the management of VLU. Statistically significant results were also noted when comparing average initial wound area and average wound area after completing the CTP application series, with large effect sizes.
Of the 122 healed wounds, only 36.1% were noted as healed after the fourth CTP application; 74.59% were healed after the seventh CTP application. It is important to note that had CTP treatment been stopped after the fourth CTP application, 63.9% of the wounds being treated would have remained unhealed. Had CTP treatment been stopped after the seventh CTP application, 25.41% of the wounds being treated would have remained unhealed. Specifically, DFUs had a 28% healed rate after the fourth CTP application and a 72% healed rate after the seventh application, whereas VLUs showed a 41.67% healed rate after the fourth CTP application and a 76.39% healed rate after the seventh application.
The mean WAR at 4 weeks was 63% for the DFU cohort and 59% for the VLU cohort. Of the DFU wounds that went on to close, the median WAR at 4 weeks was 96.55%, compared with 31.23% for wounds that did not go on to close. Of the VLU wounds that went on to close, the median WAR at 4 weeks was 87.32%, compared with 53.85% for wounds that did not go on to close. Therefore, percentage WAR at 4 weeks appears to be a predictor for eventual wound closure.
The study data indicate that Black patients required an average of 6.58 skin substitute applications to achieve wound closure, whereas White patients required an average of 5.36 applications.
It is also important to note that 69.81% (n = 148) of the patients studied had diabetes mellitus, with an average HbA1c level of 7.45. Of the healed patients with diabetes, 48.65% had an HbA1c level greater than or equal to 7, and 51.35% had an HbA1c level less than 7. This suggests that although uncontrolled diabetes is thought to hinder wound healing, it does not differentiate the effectiveness of CTP on patients with uncontrolled diabetes.
Reimbursement governing bodies have cited previous prospective randomized controlled trials to determine the number of CTP applications used to manage Wagner grade 1 and 2 DFUs, with the current proposed LCD indicating an average of 4 applications to heal a wound.19 However, it is important to note that the current study is not limited to DFUs alone; it also includes VLUs, patients who use nicotine, and patients with an HbA1c level greater than 7. This population represents a real-world, evidence-based cohort rather than the idealized randomized controlled trial cohort. Patient demographics and individualized care are crucial, because different wound etiologies, comorbidities, genetic factors, financial status, and living conditions must be considered. The current study, which was conducted in the southern United States, exhibits a high prevalence of diabetes, hypertension, and both heart and kidney disease. Therefore, setting a fixed number of skin substitute applications may not be appropriate without considering these factors. The current study demonstrates that increased CTP applications lead to increased WAR and higher chances of complete wound closure in 2 wound etiologies, various patient populations, in the presence of numerous comorbidities, and in patients with an HbA1c level greater than 7. The current study also evaluated multiple characteristics of healed DFUs and VLUs.
Substantial evidence is crucial to ensure the establishment of proper guidelines concerning the approved number of CTP applications for the management of Wagner grade 1 and 2 DFUs and VLUs. Several systematic reviews have noted that CTP applications have effectively reduced wound sizes of DFUs.12,14-17,20 The current study helps identify WAR and healing rates with each CTP application when managing DFUs and VLUs within a 16-week period. Particularly, this study determined average WAR with CTP treatments for DFUs and VLUs. Continued review of evidence-based research can provide additional insight into the optimal number of CTP applications necessary to effectively reduce DFU and VLU size. The valuable results of these practical treatments for DFUs and VLUs should be validated in further studies with robust methodology and larger sample sizes to enhance the care of patients with refractory DFUs and VLUs and to ensure inclusion of a sufficient number of CTP applications in future coverage guidelines.
A reliance upon solely vendor-sponsored randomized clinical trials has historically stifled innovation. The Centers for Medicare & Medicaid Services has reiterated this concept with actions to revise the coverage with evidence development process. Diminishing the value of retrospective studies defies the intention of Section 3022 of the 21st Century Cures Act, which calls for the use of real-world data in generating coverage policies that affect real-world patients.22
Limitations
The current study has several limitations. A larger sample size is necessary to strengthen the effectiveness and bolster the statistical power of the analysis. Additionally, this analysis included only Medicare patients, because most of the patients receiving CTPs at the time of data collection had Medicare insurance. As a result, the majority of the sample was aged 65 years or older. Including alternative insurance carriers in future studies will result in larger sample sizes and a broader range of age groups, which are necessary to provide more generalized findings of CTP therapy in the management of DFU and VLU.
The variable “time to heal” was not applicable for all patients in this review, because not all wounds had healed by the completion of the CTP application series. Standardized reporting should be in place to obtain more accurate time frames and results. Given the aim of the study, wound sizes were evaluated for a maximum of 16 weeks. The variable time to heal could also provide evidence regarding the predictability of covariates after completion of a CTP application series for DFU or VLU.
Data collection is another limitation of this study. All charts were reviewed through automated reports, and individual charts were manually reviewed. The accuracy of medical coding was essential to obtain the analyzed sample. Wound size is another limitation of this study, because only wounds between 0 and 25 cm2 in size were included for analysis. Additional studies may be needed to evaluate both the efficacy of CTPs for wounds larger than 25 cm2 and alternative advanced modalities for improving wound healing rates. Only 2 chronic wound etiologies were evaluated for this study. Prospective studies evaluating the number of CTP applications and healing rates in various chronic wound etiologies, such as pressure ulcers and burn wounds, would provide a robust overview of CTP efficacy in the wound care field. However, the vast majority of the patients in the current study had full-thickness wounds, with some even involving bone and tendon.
Healed wound characteristics in relation to the type of CTPs applied were a considerable constraint of this study. Of the wounds that healed during the CTP application series, the type of CTP used varied considerably. A slight majority of the sample received several CTPs throughout the application series; thus, the data do not support a generalization favoring any particular CTP over others. Additional research comparing CTPs is necessary due to the abundant Food and Drug Administration–approved products available for managing chronic wounds. Research comparing the efficacy of CTP monotherapy is needed to ensure evidence-based decisions are made when determining the number of applications required. No attempt was made, nor was it possible, to control for the type of CTP used other than for inclusion by the local MAC.
Future studies should meticulously consider and comprehensively report appropriate outcome analyses to mitigate the risk of bias and enhance evidence quality. Studies should also explore the cost-effectiveness of using specific CTPs to reduce wound sizes of DFUs and VLUs. Cost is a compelling area of study, because it is a common barrier to the use of nonstandard treatment. Forthcoming evaluations should explore cost issues, because these often serve as common barriers that hinder the adoption of new treatments over established conventional standards.
Conclusion
The management of Wagner grade 1 and 2 DFUs and VLUs presents significant health care challenges globally, necessitating comprehensive treatment strategies to alleviate patient suffering and reduce chronic wound morbidity and mortality. This 6-year, real-world analysis of Medicare patients receiving CTP therapy in conjunction with SOC for the management of DFUs and VLUs in a non-HOPD setting demonstrates significant reduction in average initial wound sizes after completing a CTP application series. Results of this study could be used to advise on the average number of CTP applications required in the effective management of Wagner grade 1 and 2 DFUs and VLUs. Future studies should explore the number of CTP applications required to manage other wound types to potentially enhance the quality of life of these patients, as well as to reduce amputation rates, hospital admissions, and potentially life-threatening complications.
Acknowledgments
Authors: Shaun Carpenter, MD, CWSP; Angelina Ferguson, DNP, FNP, CWS; Devinna Bahadur, DNP, MSN Ed, AGACNP-BC; Amanda Estapa, ACNP-BC, CWS; and Jamie Bahm, RHIA, CCS
Affiliation: MedCentris Wound Healing Institute, Hammond, LA
Acknowledgement: We would like to acknowledge Ms Sadie L. Burst, Intern and Bachelor of Science candidate at the University of Alabama at Birmingham, for her dedication and contributions to completing this manuscript.
Disclosure: The authors disclose no financial or other conflicts of interest.
Correspondence: Angelina Ferguson, DNP; Clinical Research Practitioner, MedCentris Wound Healing Institute, Clinical, 16065 Lamonte Drive, Hammond, LA 70403; angelina.ferguson@medcentris.com
Manuscript Accepted: June 5, 2024
Recommended Citation
Carpenter S, Ferguson A, Bahadur D, Estapa A, Bahm J. Evaluating the number of cellular and/or tissue-based product applications required to treat diabetic foot ulcers and venous leg ulcers in non-hospital outpatient department settings. Wounds. 2024;36(8):245-254. doi:10.25270/wnds/24092
References
1. Brennan MB, Tan TW, Schechter MC, Fayfman M. Using the National Institute on Minority Health and Health Disparities framework to better understand disparities in major amputations. Semin Vasc Surg. 2023;36(1):19-32. doi:10.1053/j.semvascsurg.2023.01.002
2. Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. doi:10.1186/s13047-020-00383-2
3. Centers for Disease Control and Prevention. National diabetes statistics report. 2024. Accessed May 5, 2024. https://www.cdc.gov/diabetes/data/statistics-report/index.html#print.
4. Armstrong DG, Tettelbach WH, Chang TJ, et al. Observed impact of skin substitutes in lower extremity diabetic ulcers: lessons from the Medicare database (2015-2018). J Wound Care. 2021;30(Sup7):S5-S16. doi:10.12968/jowc.2021.30.Sup7.S5
5. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293(2):217-228. doi:10.1001/jama.293.2.217
6. Probst S, Saini C, Gschwind G, et al. Prevalence and incidence of venous leg ulcers: a systematic review and meta-analysis. Int Wound J. 2023;20(9):3906-3921. doi:10.1111/iwj.14272
7. Serena TE, Orgill DP, Armstrong DG, et al. A multicenter, randomized, controlled, clinical trial evaluating dehydrated human amniotic membrane in the treatment of venous leg ulcers. Plast Reconstr Surg. 2022;150(5):1128-1136. doi:10.1097/PRS.0000000000009650
8. Schmiedova I, Dembickaja A, Kiselakova L, Nowakova B, Slama P. Using of amniotic membrane derivatives for the treatment of chronic wounds. Membranes (Basel). 2021;11(12):941. doi:10.3390/membranes11120941
9. Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care (New Rochelle). 2021;10(5):281-292. doi:10.1089/wound.2021.0026
10. Norman G, Westby MJ, Rithalia AD, Stubbs N, Soares MO, Dumville JC. Dressings and topical agents for treating venous leg ulcers. Cochrane Database Syst Rev. 2018;6(6):CD012583. doi:10.1002/14651858.CD012583.pub2
11. Vecin NM, Kirsner RS. Skin substitutes as treatment for chronic wounds: current and future directions. Front Med (Lausanne). 2023;10:1154567. doi:10.3389/fmed.2023.1154567
12. Kelangi SS, Theocharidis G, Veves A, et al. On skin substitutes for wound healing: current products, limitations, and future perspectives. World Scientific. 2020;08:01n02. doi:10.1142/S2339547820300012
13. Mohammed YA, Farouk HK, Gbreel MI, et al. Human amniotic membrane products for patients with diabetic foot ulcers. Do they help? A systematic review and meta-analysis. J Foot Ankle Res. 2022;15(1):71. doi:10.1186/s13047-022-00575-y
14. Olsson M, Järbrink K, Divakar U, et al. The humanistic and economic burden of chronic wounds: a systematic review. Wound Repair Regen. 2019;27(1):114-125. doi:10.1111/wrr.12683
15. O’Meara S, Al-Kurdi D, Ologun Y, Ovington LG, Martyn-St James M, Richardson R. Antibiotics and antiseptics for venous leg ulcers. Cochrane Database Syst Rev. 2014;2014(1):CD003557. doi:10.1002/14651858.CD003557.pub5
16. Bay C, Chizmar Z, Reece EM, et al. Comparison of skin substitutes for acute and chronic wound management. Semin Plast Surg. 2021;35(3):171-180. doi:10.1055/s-0041-1731463
17. Wardhana A, Valeria M. Efficacy of skin substitutes for management of acute burn cases: a systematic review. Ann Burns Fire Disasters. 2022;35(3):227-236.
18. Tettelbach W, Cazzell S, Reyzelman AM, Sigal F, Caporusso JM, Agnew PS. A confirmatory study on the efficacy of dehydrated human amnion/chorion membrane dHACM allograft in the management of diabetic foot ulcers: a prospective, multicentre, randomised, controlled study of 110 patients from 14 wound clinics. Int Wound J. 2019;16(1):19-29. doi:10.1111/iwj.12976
19. Centers for Medicare and Medicaid Services. Skin substitute grafts/cellular and tissue-based products for the treatment of diabetic foot ulcers and venous leg ulcers. Medicare Coverage Database. Accessed April 25, 2024. Retrieved May 5, 2024. https://www.cms.gov/medicare-coverage-database/view/lcd.aspx?lcdid=39870&ver=4. 2024.
20. Chandler LA, Alvarez OM, Blume PA, et al. Wound conforming matrix containing purified homogenate of dermal collagen promotes healing of diabetic neuropathic foot ulcers: comparative analysis versus standard of care. Adv Wound Care (New Rochelle). 2020;9(2):61-67. doi:10.1089/wound.2019.1024
21. Lakmal K, Basnayake O, Hettiarachchi D. Systematic review on the rational use of amniotic membrane allografts in diabetic foot ulcer treatment. BMC Surg. 2021;21(1):87. doi:10.1186/s12893-021-01084-8
22. 21st Century Cures Act, Pub L No. 114-255. Accessed May 5, 2024. https://www.govinfo.gov/app/details/PLAW-114publ255
