



Effectiveness of Negative Pressure Wound Therapy in Patients With Challenging Wounds: A Systematic Review and Meta-analysis
Abstract
Introduction. Controversy exists regarding the use of NPWT for wound healing. Objective. This study assessed the effectiveness of NPWT compared with conventional treatment in the management of different wound types, including acute and chronic wounds. Materials and Methods. PubMed, Cochrane Central Register of Controlled Trials, Scopus, EMBASE, EBSCO, Ovid, and Web of Science were searched, from database inception up to October 2021, for relevant studies comparing NPWT with conventional treatment for wound healing. Primary outcomes included time to healing, wound healing rate, and duration of treatment. Secondary outcomes included adverse events, length of hospital stay, and 30-day mortality rate. Pooled analysis of the outcomes data is presented as SMD (95% CI) for continuous data and OR (95% CI) for dichotomous data. Results. Twenty-four studies (3064 patients) were included in the meta-analysis. NPWT was associated with shorter time to healing (SMD, −0.79; 95% CI, −1.22 to −0.37), shorter duration of treatment (SMD, −1.24; 95% CI, −1.92 to −0.56), and higher rate of wound healing (OR, 2.05; 95% CI, 1.49-2.83) compared with control. NPWT was also associated with a lower incidence of adverse events (OR, 0.42; 95% CI, 0.23-0.77) and a lower 30-day mortality rate (OR, 0.25; 95% CI, 0.12-0.56). There were no significant differences between NPWT and control regarding hospital stay (SMD, −0.52; 95% CI, −1.06 to 0.03). Conclusions. NPWT is seemingly associated with better wound healing outcomes compared with conventional therapy. However, the data should be interpreted with substantial caution given limitations such as high heterogeneity between studies and the small sample size of the included studies.
Abbreviations
CI, confidence interval; NPWT, negative pressure wound therapy; OR, odds ratio; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT, randomized controlled trial; SMD, standardized mean difference.
Introduction
Wound healing and wound care, especially of challenging and resistant wounds such as diabetic foot wounds and postoperative infected wounds, have always been a point of interest for many physicians and surgeons in various specialties.1 Advances in medicine have resulted in the development of new methods of wound management. Over the past 2 decades, the use of NPWT has evolved, and it has become an important and popular method of wound management.2
NPWT, also known as vacuum-assisted wound closure, reportedly has been used in many types of wounds, such as surgical wounds, chronic wounds, and open infected wounds, as well as skin grafts.3,4 The mechanism of NPWT involves the creation of a sealed environment around the wound by placing a foam dressing in the wound cavity and covering it with an adhesive drape, then applying negative pressure in that sealed environment using a pump.5
The means by which applying negative pressure around the wound accelerates healing are still not thoroughly understood, but they may involve reducing edema, improving blood flow, mechanical approximation of edges, and enhancing granulation tissue formation. Although the cost of NPWT is higher than conventional wound management, NPWT is more cost-effective overall because it accelerates wound healing, thus shortening length of hospital stay and absence from work or school.6
The use of NPWT is favored based on clinical experience and scientific research.7 Previous clinical trials that studied this technique usually evaluated the role of NPWT in a specific wound type. In this systematic review, uses of NPWT in multiple wound types were included in the search and were analyzed with the goal of improving decision-making regarding wound management in various situations.
Materials and Methods
All steps of this study were conducted in strict accordance with the Cochrane Handbook for Systematic Reviews of Interventions and PRISMA statement guidelines.8,9
Literature search strategy
PubMed, Cochrane Central Register of Controlled Trials, Scopus, EMBASE, EBSCO, Ovid, and Web of Science were searched, from database inception up to October 2021, for studies comparing NPWT with control (ie, conventional treatment). The following keywords were used: (“negative pressure therapy” OR “topical negative pressure” OR TNP, OR NPWT OR “vacuum-assisted closure” OR V.A.C. AND “wound infection” OR “infected wound”). Additionally, the reference lists of identified articles were checked manually.
Eligibility criteria
Studies that met the following criteria were included. The population comprised adult patients with different types of wounds. The intervention comprised negative pressure, topical negative pressure, or vacuum-assisted wound closure. The comparator comprised normal dressing, conventional dressing, or any other control. Primary outcomes included time to healing, duration of treatment, hospital duration, and incidence of wound healing. Secondary outcomes included serious adverse events, secondary wound infection, wound breakdown, recurrence, blood transfusion and/or bleeding, and sepsis. RCTs and comparative studies were included.
Exclusion criteria included animal models, reviews, case reports, case series, non-English language articles, and duplicate references.
Study selection
First, title and/or abstract screening was conducted for eligibility in the current study. Second, full-text screening was conducted. Each step was performed by 3 independent reviewers (M.S.A.S., Y.E., A.H.A.), and disagreements were resolved by consensus.
Data extraction
Requisite data were extracted by 3 independent authors (A.R.A., A.M., K.T.) into a data extraction form. The extracted data included the following items: baseline characteristics of enrolled patients, general characteristics of study design, and included outcomes.
In case of a missing mean or standard deviation, the authors of the current study calculated those values using the equations in Hozo et al10 or provided in the Cochrane Handbook for Systematic Reviews of Interventions.8
Assessment of risk of bias
The Cochrane collaboration tool was used to assess the risk of bias of included RCTs.8 Risk of bias assessment included sequence generation, allocation sequence concealment, blinding of participants and personnel, blinding of outcomes assessment, incomplete outcomes data, selective outcomes reporting, and other potential sources of bias. The judgment of the authors of the current study was categorized as “low risk,” “high risk,” or “unclear risk” of bias. The Newcastle-Ottawa scale was used to evaluate the quality of observational studies, and each included study was assessed based on reporting of 3 essential domains: (1) selection of the study subjects, (2) comparability of groups based on demographic characteristics and important potential confounders, and (3) ascertainment of the included outcome (exposure and/or treatment).12
Data synthesis
Continuous data were pooled using a SMD (95% CI). Dichotomous data were pooled to calculate the OR (95% CI). R software (version 4.9-0; The R Project for Statistical Computing) for Windows (Microsoft) was used during data synthesis.
Heterogeneity was assessed by visual inspection of forest plots and measured by the Q statistic and the I2 statistic. Significant statistical heterogeneity was indicated by a Q statistic P value less than .1 or by I2 greater than 50%. Random-effect models were used when significant heterogeneity was found, and the fixed-effect model was used in cases without significant heterogeneity. Subgroup analysis and sensitivity analysis were used to resolve heterogeneity.
Publication bias
The Egger test was used to assess publication bias for outcomes reported in more than 10 studies.13
Results
Literature search and study selection
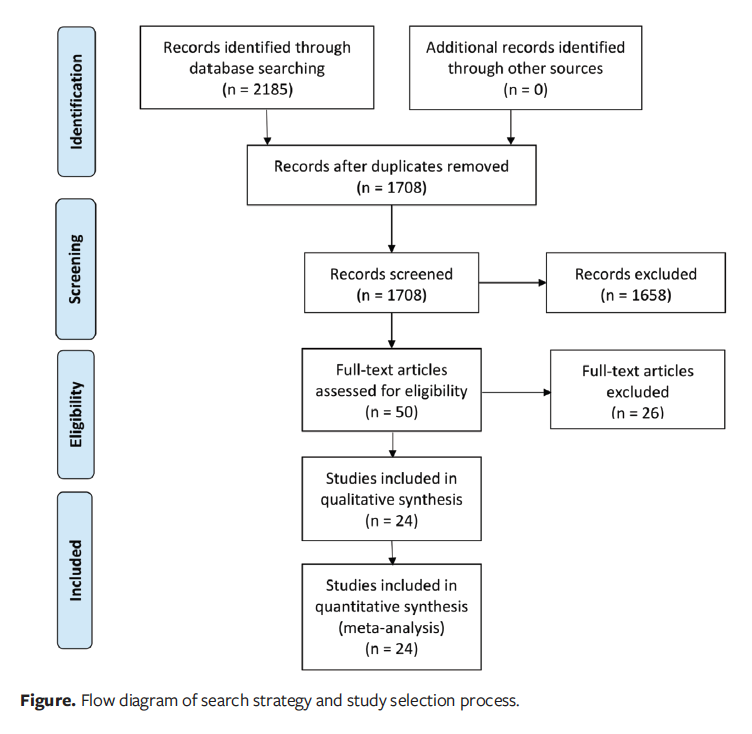
The literature search of databases yielded 1708 unique records. After title and abstract screening, 50 articles were retrieved and screened for eligibility. Of these, 24 studies were included in the meta-analysis. The study selection process is shown in the PRISMA flow diagram (Figure).
Characteristics of studies and risk
of bias
Characteristics of the included studies are summarized in Table 1. A total of 24 studies (15 RCTs6,14–27 and 9 cohort studies28–36) enrolling 3064 patients were included; of these, 1574 patients underwent NPWT and 1490 received conventional dressing. Apelqvist et al6 and Armstrong and Lavery16 were conducted on the same study group. The comparator control group treatments included standard moist wound dressings, advanced moist wound therapy, modern wound dressings, and conventional wound care techniques. Follow-up ranged from 10 days to 24 months. There were no studies involving children; the average age of the included patients was 56.2 years. The included studies were geographically limited; all were from high- and upper-middle−income countries, with 7 conducted in the Netherlands, 5 in the United States, 3 in China, 2 in Switzerland, and 1 each in Korea, Iran, Italy, Australia, Germany, France, and Turkey.
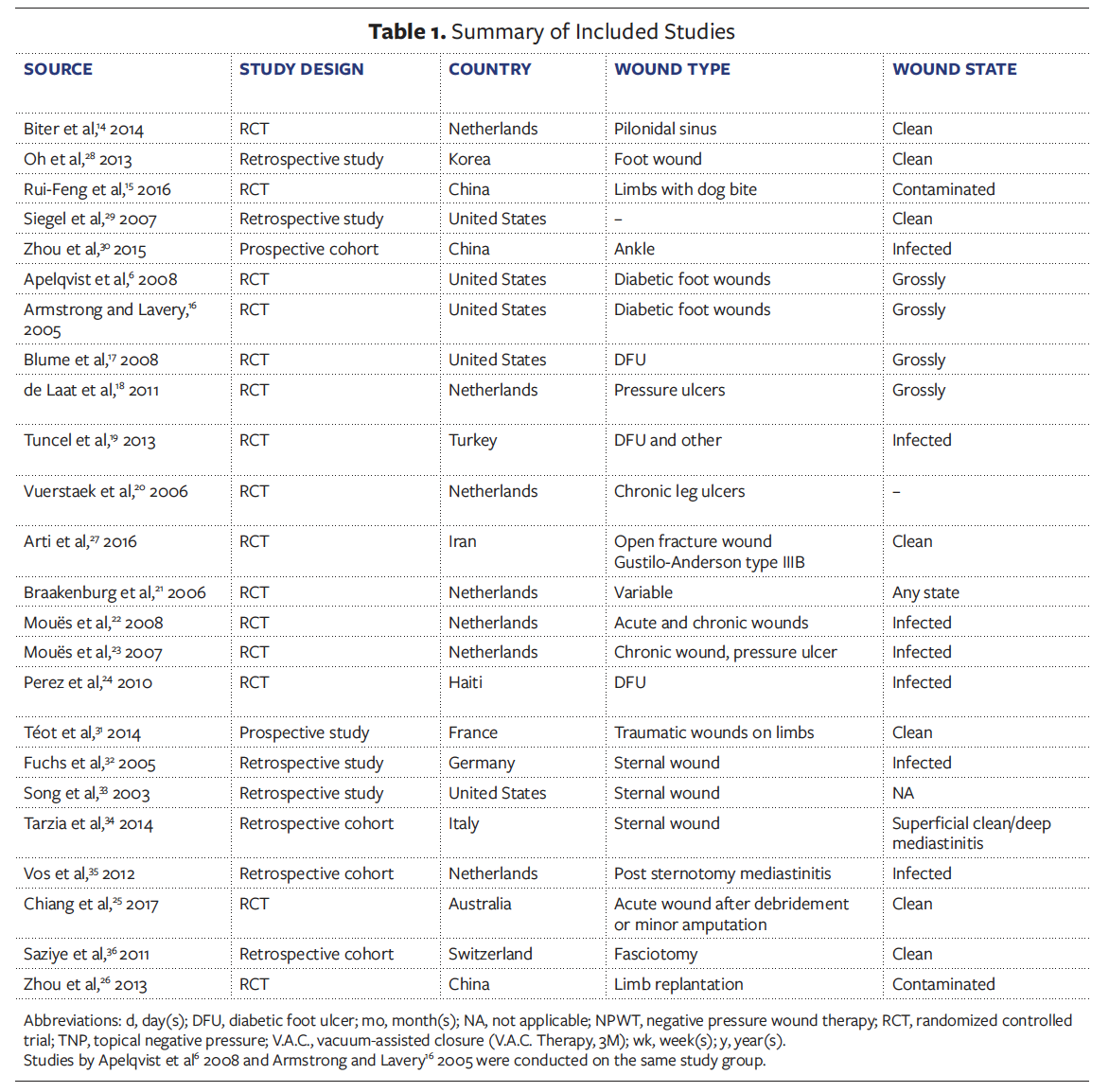
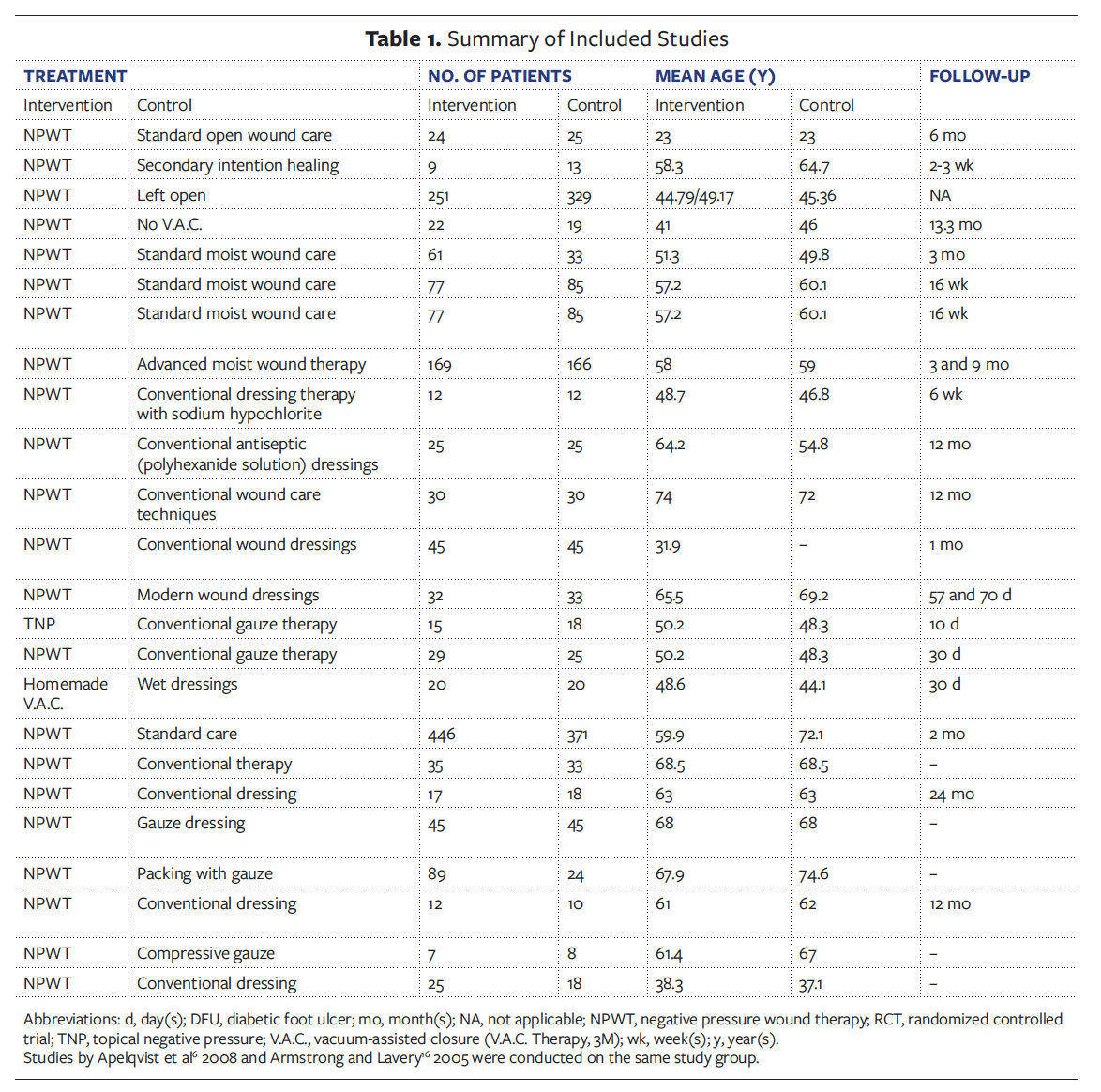
Different wound types were included in the studies, such as acute wounds (5 studies), chronic wounds (5 studies), fracture wounds (2 studies), vascular wounds (2 studies), sternal wounds (4 studies), and others (6 studies). The risk of bias in included studies was acceptable according to the Cochrane risk of bias assessment and the Newcastle-Ottawa scale (Table 4).
Outcomes
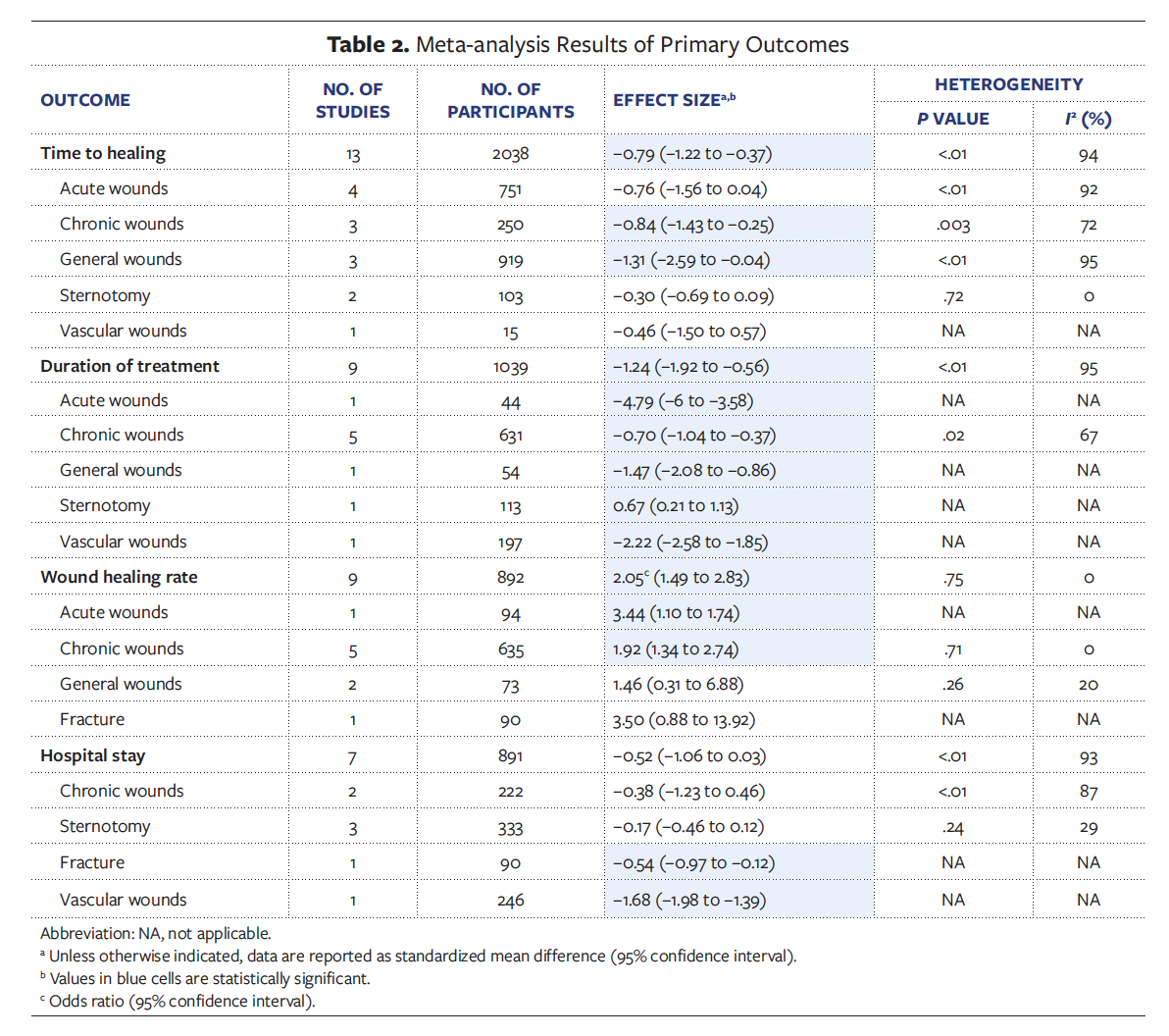
Primary outcomes. Compared with control, meta-analysis showed that NPWT was associated with shorter time to healing (SMD, −0.79; 95% CI, −1.22 to −0.37), shorter duration of treatment (SMD, −1.24; 95% CI, −1.92 to −0.56), and increased incidence of wound healing (OR, 2.05; 95% CI, 1.49-2.83). However, there was no significant difference between NPWT and control regarding hospital stay (SMD, −0.52; 95% CI, −1.06 to 0.03) (Table 2).
Secondary outcomes. Meta-analysis showed that NPWT was associated with decreased incidence of serious adverse events (OR, 0.42; 95% CI, 0.23-0.77) and lower 30-day mortality rate (OR, 0.25; 95% CI, 0.12-0.56) compared with control. There were no significant differences between NPWT and control in terms of secondary wound infection (OR, 1.00; 95% CI, 0.76-1.31), amputation (OR, 0.44; 95% CI, 0.15-1.24), wound breakdown (OR, 1.08; 0.46-2.57), recurrence (OR, 0.47; 95% CI, 0.22-1.02), blood transfusion/bleeding (OR, 1.31; 95% CI, 0.43–4.01), and sepsis (OR, 0.70; 95% CI, 0.29–1.69) (Table 3).
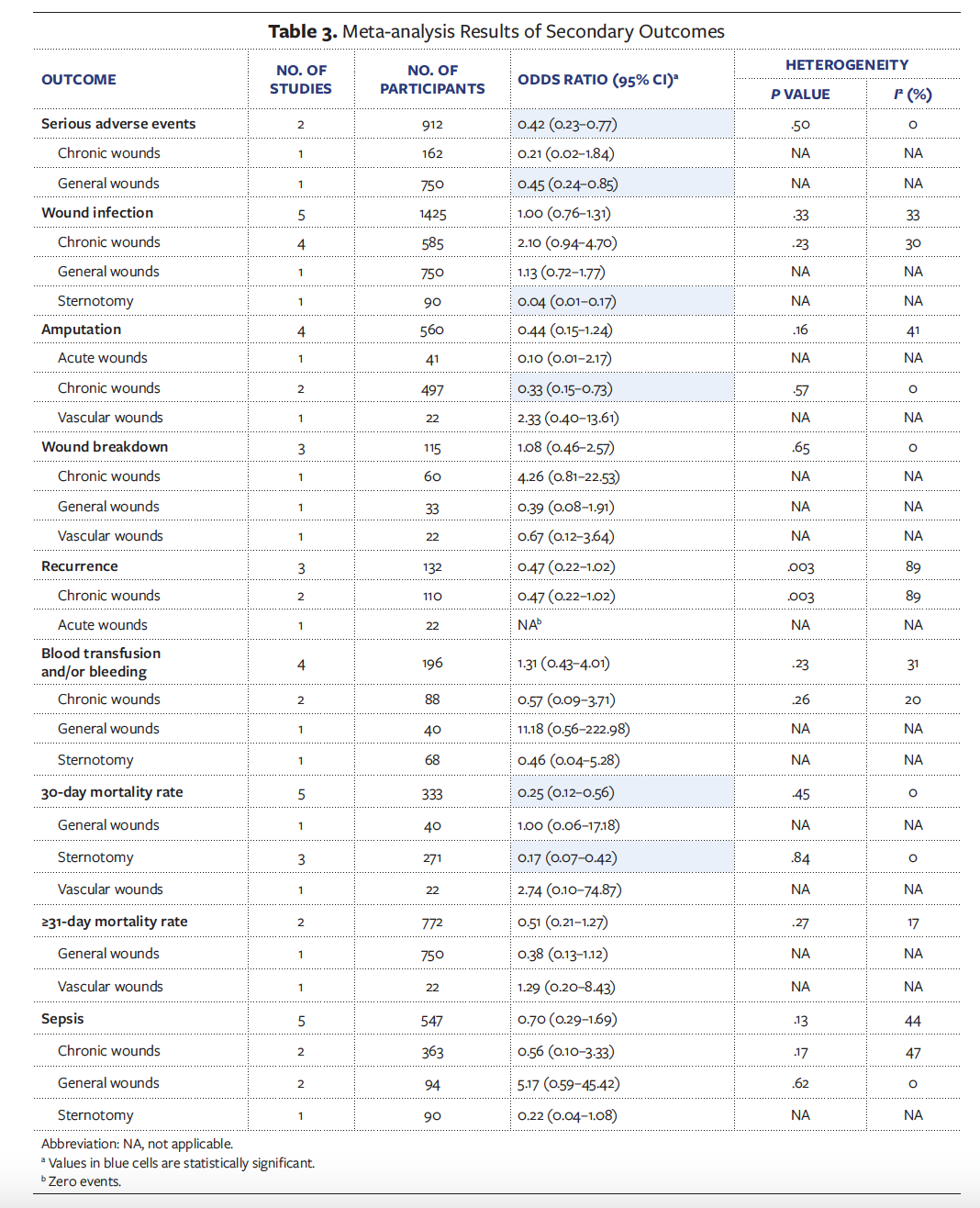
Subgroup analysis. Subgroup analysis according to wound type was consistent with the overall analysis in most outcomes. Regarding time to healing, there was no significant difference between NPWT and control in acute wounds (SMD, −0.76; 95% CI, −1.56 to 0.04), sternotomy (SMD, −0.30; 95% CI, −0.69 to 0.09), and vascular wounds (SMD, −0.46; 95% CI, −1.50 to 0.57). Regarding wound healing rate, no significant difference was detected between the compared groups in terms of general surgery wounds (OR, 1.46; 95% CI, 0.31–6.88) and fracture wounds (OR, 3.50; 95% CI, 0.88–13.92) (Table 2). In patients with chronic wounds, NPWT was associated with a lower rate of amputation compared with control (OR, 0.33; 95% CI, 0.15–0.73) (Table 3).
Publication bias. No significant publication bias was detected according to the Egger test (P < .1).
Discussion
Over the past 2 decades, NPWT has been commonly used in the management of various types of medical and surgical wounds. NPWT enhances local blood flow and proliferation of tissues, and it reduces soft tissue bacterial infection and local edema.28 Two types of tissue deformation occur during NPWT: macrodeformation (ie, wound contracture) and microdeformation (at the microscopic level).35,36 These types of tissue deformation are thought to mostly influence the early stages of injury healing—that is, inflammation and proliferation. NPWT systems draw wound margins together by generating subatmospheric pressure in the whole wound bed.37 The tissue surface is strained by an estimated 5% to 20% by the NPWT; negative pressure on the wound bed leads to wound surface undulations, and tissue blebs are drawn into the pores of the dressing. The mechanical pressure transmitted to the tissues promotes the healing cascade, which comprises migration, differentiation, granulation tissue promotion, angiogenesis, and epithelialization.38 Reduction in local edema results in removal of excess extracellular fluid, leading to reduced capillary hydrostatic compression and reduction in the required diffusion distance.39 NPWT prevents inflammatory cytokines and proteases, which may worsen healing processes by extracting excess wound fluid.40 Additionally, as NPWT extracts wound exudates, it aids in keeping moist wound environments clean, and as such, fewer dressing changes are necessary.
Regarding the time of wound healing, the findings of the present study demonstrated that NPWT was associated with a shorter time to healing compared with control (SMD, −0.79; 95% CI, −1.22 to −0.37). The shortest duration of healing was observed in general wounds (SMD, −1.31; 95% CI, −2.59 to −0.04), chronic wounds (SMD, −0.84; 95% CI, −1.43 to −0.25), and acute wounds (SMD, −0.76; 95% CI, −1.56 to −0.04). There was no significant difference between infected and clean wounds regarding time to healing. These findings confirm that NPWT results in faster granulation tissue formation and faster surface area reduction during the first week of treatment. Liu et al41 reported that the median time to healing was 21 days shorter with NPWT versus moist dressings in postoperative wounds (hazard ratio, 1.91; 95% CI, 1.21–2.99).
Regarding the incidence of wound healing, the current results showed that the application of NPWT significantly increased the incidence of wound healing (2 times) compared with conventional methods (OR, 2.05; 95% CI, 1.49–2.83). This incidence increased to 3 times that of control in acute wounds (OR, 3.44; 95% CI, 1.10–1.74) and fracture wounds (OR, 3.50; 95% CI, 0.88–13.92). This may positively affect cost-effectiveness and the duration of hospitalization. Similarly, Liu et al41 reported an increased number of healed wounds in the NPWT group compared with the dressings group in persons with diabetic foot ulcers and postoperative wounds.
Concerning length of hospital stay, there was no significant difference between NPWT and control (SMD, −0.52; 95% CI, −1.06 to 0.03). Li et al42 showed that NPWT did not prolong length of hospital stay compared with control (SMD, −0.38; 95% CI, −0.78 to 0.02). In contrast, Antoniou et al43 reported that NPWT was associated with shorter hospital stay compared with control (SMD, −2.14; 95% CI, −3.78 to 0.49). However, Antoniou et al43 noted that this result was based on data from 2 studies; thus, data are insufficient to confirm this finding.
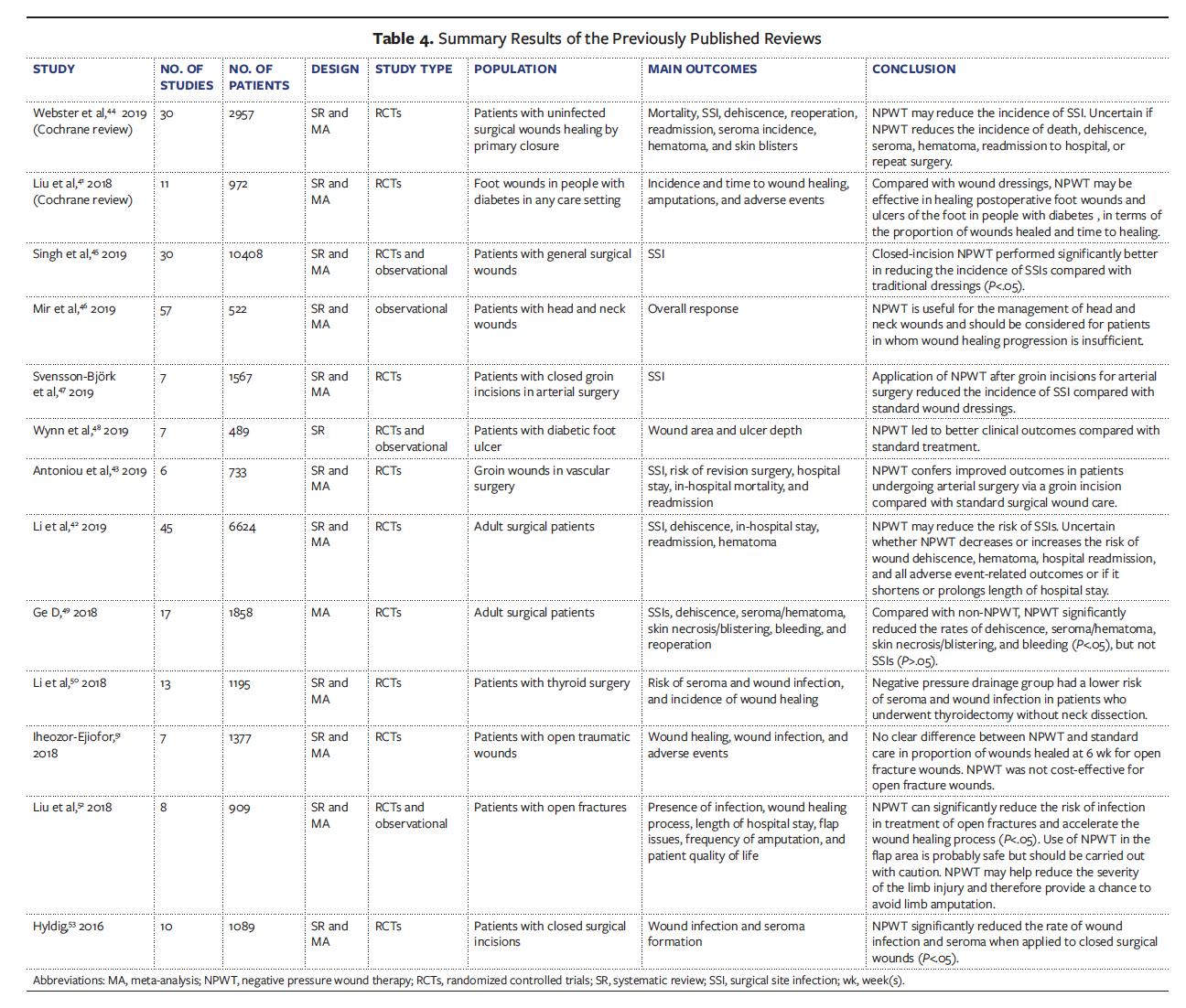
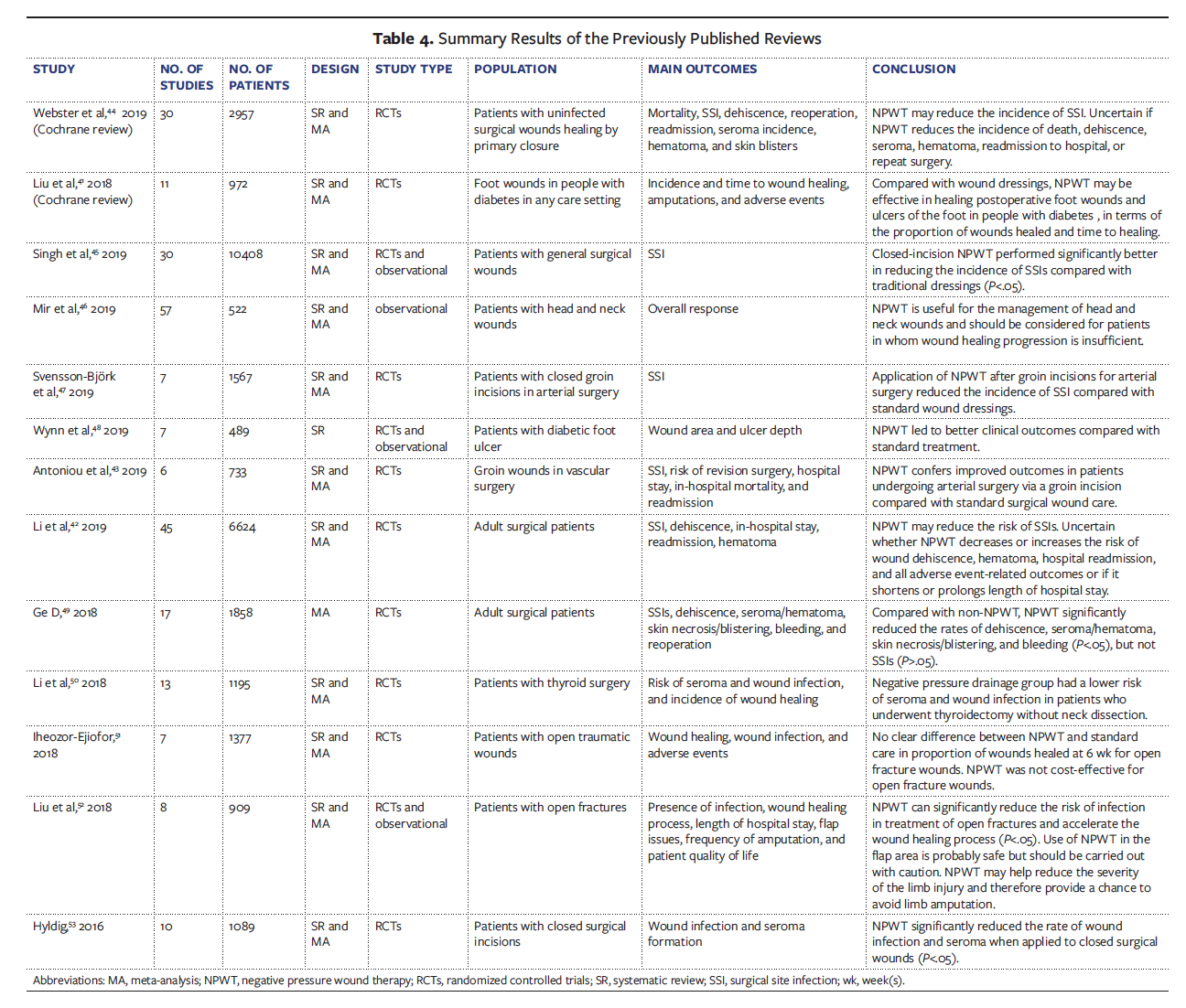
In terms of safety, the present meta- analysis demonstrated that NPWT was associated with a lower incidence of serious adverse events (OR, 0.42; 95% CI, 0.23–0.77) and lower 30-day mortality rate (OR, 0.25; 95% CI, 0.12–0.56) compared with control. However, Li et al42 reported that NPWT significantly increased the risk of all adverse event-related outcomes (OR, 3.21; 95% CI, 1.17–8.78). Concerning risk of death, Webster et al44 reported a risk ratio of 0.63 (95% CI, 0.25–1.56) with NPWT compared with standard dressing. Of note, the results of the present meta-analysis agreed with those of previous meta- analyses in some outcomes but differed in others. This may be owing to the different number of included studies; the present study included more recent studies. Table 4 shows the comparison of the current study with the previously published review articles.45–53
In the current study, the authors’ assessments of the risk of bias for the previously reported domains found that all studies showed minor limitations in study design and implementation. However, the blinding of NPWT is quite difficult or even impossible, and subsequently there was uncertainty about allocation concealment and blinding of outcomes assessment. Statistical heterogeneity was high for the primary outcomes, with the exception of the incidence of wound healing; however, the authors of the current study do not believe this affected the results of the study. This heterogeneity can be explained by the large variation between the sample sizes of the included studies, which ranged from 15 patients to 817 patients; the different methods of NPWT application; different intensity of negative pressure; geographical variation; and various wound states, whether infected or clean.
Limitations
Procedures were clearly defined to avoid prospective bias in the review process. The authors of the present study conducted a careful literature search and used transparent and reproducible methods. Three reviewers were involved in all steps of screening, data extraction, and quality assessment to avoid potential bias. Studies published in publications outside the search strategy or inclusion criteria may have been missed, however. Some studies did not include the information necessary to assess study quality; therefore, the authors of the present study may have underestimated the quality of these studies.
Conclusions
The current evidence suggests that NPWT has a promising role in reducing duration of treatment and time to wound healing, and in increasing the incidence of healing. Moreover, NPWT was associated with a lower incidence of serious adverse events and mortality rate. Future studies should assess the prophylactic role of NPWT in surgical incisions to minimize or avoid surgical site infection. Further research is recommended to evaluate the clinical effectiveness and cost-effectiveness of NPWT, which is a priority for patients and health professionals.
Acknowledgments
Authors: Mohamed S.A. Shehata, MBBCh1,2; Eshak Bahbah, MBBCh3; Yousef El-Ayman, MD1; Ahmed H. Abdelkarim, MBBCh1; Ahmed R. Abdalla, MD4; Ahmed Morshedy, MBBCh5; Khaled Turkmani, MD6; Ishith Seth, MD7; and Nimish Seth, MD8
Affiliations: 1Faculty of Medicine, Zagazig University, Zagazig, Egypt; 2Nasr City Insurance Hospital, Cairo, Egypt; 3Faculty of Medicine, Al-Azhar University, Damietta, Egypt; 4Faculty of Medicine, Mansoura University, Mansoura, Egypt; 5Faculty of Medicine, Kafrelsheikh University, Kafrelsheikh, Egypt; 6Faculty of Medicine, Damascus University, Damascus, Syria; 7Illawarra Shoalhaven Local Health District, Wollongong, Australia; 8Department of Orthopaedics, The Alfred Hospital, Melbourne, Australia
Disclosure: The authors disclose no financial or other conflicts of interest.
Correspondence: Mohamed S.A. Shehata, MBBCh, Nasr City Insurance Hospital, Cairo, Egypt, 44771; mohamed.shehata6@outlook.com
References
1. Amalsadvala T, Swaim SF. Management of hard-to-heal wounds. Vet Clin North Am Small Anim Pract. 2006;36(4):693-711. doi:10.1016/j.cvsm.2006.02.002
2. Thompson JT, Marks MW. Negative pressure wound therapy. Clin Plast Surg. 2007;34(4):673-684. doi:10.1016/j.cps.2007.07.005
3. Gupta S. Optimal use of negative pressure wound therapy for skin grafts. Int Wound J. 2012;9(Suppl 1):40-47. doi:10.1111/j.1742-481X.2012.01019.x
4. Masumoto K, Nagata K, Oka Y, et al. Successful treatment of an infected wound in infants by a combination of negative pressure wound therapy and arginine supplementation. Nutrition. 2011;27(11-12):1141-1145. doi:10.1016/j.nut.2011.01.006
5. Argenta LC, Morykwas MJ. Vacuum-assisted closure: a new method for wound control and treatment: clinical experience. Ann Plast Surg. 1997;38(6):563-576.
6. Apelqvist J, Armstrong DG, Lavery LA, Boulton AJM. Resource utilization and economic costs of care based on a randomized trial of vacuum- assisted closure therapy in the treatment of diabetic foot wounds. Am J Surg. 2008;195(6):782-788. doi:10.1016/j.amjsurg.2007.06.023
7. Malmsjö M, Borgquist O. NPWT settings and dressing choices made easy. Wounds Int. 2010;1(3):1-6.
8. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions. Vol 4. John Wiley & Sons; 2011.
9. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372. doi:10.1136/bmj.n71
10. Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5(1):13. doi:10.1186/1471-2288-5-13
11. Altman DG. Standard deviations and standard errors. BMJ. 2005;331(7521):903-903. doi:10.1136/bmj.331.7521.903
12. Stang A. Critical evaluation of the Newcastle- Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603-605. doi:10.1007/s10654-010-9491-z
13. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-634. doi:10.1136/bmj/315.7109.629
14. Biter LU, Beck GMN, Mannaerts GHH, Stok MM, van der Ham AC, Grotenhuis BA. The use of negative-pressure wound therapy in pilonidal sinus disease. Dis Colon Rectum. 2014;57(12):1406-1411. doi:10.1097/DCR.0000000000000240
15. Rui-Feng C, Li-Song H, Ji-Bo Z, Yi-Qing J, Yu-Jie L, Yi S. Negative pressure wound therapy for serious dog bites of extremities: a prospective randomized trial. Am J Emerg Med. 2016;34(6):1006-1010. doi:10.1016/j.ajem.2016.02.043
16. Armstrong DG, Lavery LA, Diabetic Foot Study Consortium. Negative pressure wound therapy after partial diabetic foot amputation: a multicentre, randomised controlled trial. Lancet. 2005;366(9498):1704-1710. doi:10.1016/S0140-6736(05)67695-7
17. Blume PA, Walters J, Payne W, Ayala J, Lantis J. Comparison of negative pressure wound therapy using vacuum-assisted closure with advanced moist wound therapy in the treatment of diabetic foot ulcers: a multicenter randomized controlled trial. Diabetes Care. 2008;31(4):631-636. doi:10.2337/dc07-2196
18. de Laat EHEW, van den Boogaard MHWA, Spauwen PHM, van Kuppevelt DHJM, van Goor H, Schoonhoven L. Faster wound healing with topical negative pressure therapy in difficult-to-heal wounds: a prospective randomized controlled trial. Ann Plast Surg. 2011;67(6):626-631. doi:10.1097/SAP.0b013e31820b3ac1
19. Tuncel U, Erkorkmaz Ü, Turan A. Clinical evaluation of gauze-based negative pressure wound therapy in challenging wounds. Int Wound J. 2013;10(2):152-158. doi:10.1111/j.1742-481X.2012.00955.x
20. Vuerstaek JDD, Vainas T, Wuite J, Nelemans P, Neumann MHA, Veraart JCJM. State-of-the-art treatment of chronic leg ulcers: a randomized controlled trial comparing vacuum-assisted closure (V.A.C.) with modern wound dressings. J Vasc Surg. 2006;44(5):1029-1037. doi:10.1016/j.jvs.2006.07.030
21. Braakenburg A, Obdeijn MC, Feitz R, van Rooij IALM, van Griethuysen AJ, Klinkenbijl JHG. The clinical efficacy and cost effectiveness of the vacuum-assisted closure technique in the management of acute and chronic wounds: a randomized controlled trial. Plast Reconstr Surg. 2006;118(2):390-397. doi:10.1097/01.prs.0000227675.63744.af
22. Mouës CM, van Toorenenbergen AW, Heule F, Hop WC, Hovius SER. The role of topical negative pressure in wound repair: expression of biochemical markers in wound fluid during wound healing. Wound Repair Regen. 2008;16(4):488-494. doi:10.1111/j.1524-475X.2008.00395.x
23. Mouës CM, van den Bemd GJCM, Heule F, Hovius SER. Comparing conventional gauze therapy to vacuum-assisted closure wound therapy: a prospective randomised trial. J Plast Reconstr Aesthetic Surg. 2007;60(6):672-681. doi:10.1016/j.bjps.2006.01.041
24. Perez D, Bramkamp M, Exe C, von Ruden C, Ziegler A. Modern wound care for the poor: a randomized clinical trial comparing the vacuum system with conventional saline-soaked gauze dressings. Am J Surg. 2010;199(1):14-20. doi:10.1016/j.amjsurg.2008.12.029
25. Chiang N, Rodda OA, Sleigh J, Vasudevan T. Effects of topical negative pressure therapy on tissue oxygenation and wound healing in vascular foot wounds. J Vasc Surg. 2017;66(2):564-571. doi:10.1016/j.jvs.2017.02.050
26. Zhou M, Qi B, Yu A, et al. Vacuum assisted closure therapy for treatment of complex wounds in replanted extremities. Microsurgery. 2013;33(8):620-624. doi:10.1002/micr.22178
27. Arti H, Khorami M, Ebrahimi-Nejad V. Comparison of negative pressure wound therapy (NPWT) and conventional wound dressings in the open fracture wounds. Pak J Med Sci. 2016;32(1):65-69. doi:10.12669/pjms.321.8568
28. Oh BH, Lee SH, Nam KA, Lee HB, Chung KY. Comparison of negative pressure wound therapy and secondary intention healing after excision of acral lentiginous melanoma on the foot. Br J Dermatol. 2013;168(2):333-338. doi:10.1111/bjd.12099
29. Siegel HJ, Long JL, Watson KM, Fiveash JB. Vacuum-assisted closure for radiation-associated wound complications. J Surg Oncol. 2007;96(7):575-582. doi:10.1002/jso.20846
30. Zhou ZY, Liu YK, Chen HL, Liu F. Wound management with vacuum assisted closure in surgical site infection after ankle surgery. Int J Surg. 2015;17:15-18. doi:10.1016/j.ijsu.2015.03.008
31. Téot L, Guillot-Masanovic M, Miquel P, et al. Clinical impact of negative-pressure wound therapy: A 1,126-patient observational prospective study. Wound Repair Regen. 2014;22(3):341-350. doi:10.1111/wrr.12179
32. Fuchs U, Zittermann A, Stuettgen B, Groening A, Minami K, Koerfer R. Clinical outcome of patients with deep sternal wound infection managed by vacuum-assisted closure compared to conventional therapy with open packing: a retrospective analysis. Ann Thorac Surg. 2005;79(2):526-531. doi:10.1016/j.athoracsur.2004.08.032
33. Song DH, Wu LC, Lohman RF, Gottlieb LJ, Franczyk M. Vacuum assisted closure for the treatment of sternal wounds: the bridge between débridement and definitive closure. Plast Reconstr Surg. 2003;111(1):92-97. doi:10.1097/01.PRS.0000037686.14278.6A
34. Tarzia V, Carrozzini M, Bortolussi G, et al. Impact of vacuum-assisted closure therapy on outcomes of sternal wound dehiscence. Interact Cardiovasc Thorac Surg. 2014;19(1):70-75. doi:10.1093/icvts/ivu101
35. Vos RJ, Yilmaz A, Sonker U, Kelder JC, Kloppenburg GTL. Vacuum-assisted closure of post-sternotomy mediastinitis as compared to open packing. Interact Cardiovasc Thorac Surg. 2012;14(1):17-21. doi:10.1093/icvts/ivr049
36. Saziye K, Mustafa C, Ilker U, Afksendyios K. Comparison of vacuum-assisted closure device and conservative treatment for fasciotomy wound healing in ischaemia-reperfusion syndrome: preliminary results. Int Wound J. 2011;8(3):229-236. doi:10.1111/j.1742-481X.2011.00773.x
37. Fabian TS, Kaufman HJ, Lett ED, et al. The evaluation of subatmospheric pressure and hyperbaric oxygen in ischemic full-thickness wound healing. Am Surg. 2000;66(12):1136-1143.
38. Greene AK, Puder M, Roy R, et al. Microdeformational wound therapy: effects on angiogenesis and matrix metalloproteinases in chronic wounds of 3 debilitated patients. Ann Plast Surg. 2006;56(4):418-422. doi:10.1097/01.sap.0000202831.43294.02
39. Huang C, Leavitt T, Bayer LR, Orgill DP. Effect of negative pressure wound therapy on wound healing. Curr Probl Surg. 2014;51(7):301-331. doi:10.1067/j.cpsurg.2014.04.001
40. Lo Torto F, Ruggiero M, Parisi P, Borab Z, Sergi M, Carlesimo B. The effectiveness of negative pressure therapy on infected wounds: preliminary results. Int Wound J. 2017;14(6):909-914. doi:10.1111/iwj.12725
41. Liu Z, Dumville JC, Hinchliffe RJ, et al. Negative pressure wound therapy for treating foot wounds in people with diabetes mellitus. Cochrane Database Syst Rev. 2018;10(10):CD010318. doi:10.1002/14651858.CD010318.pub3
42. Li HZ, Xu XH, Wang DW, Lin YM, Lin N, Lu HD. Negative pressure wound therapy for surgical site infections: a systematic review and meta-analysis of randomized controlled trials. Clin Microbiol Infect. 2019;25(11):1328-1338. doi:10.1016/j.cmi.2019.06.005
43. Antoniou GA, Onwuka CC, Antoniou SA, Russell D. Meta-analysis and trial sequential analysis of prophylactic negative pressure therapy for groin wounds in vascular surgery. J Vasc Surg. 2019;70(5):1700-1710. doi:10.1016/j.jvs.2019.01.083
44. Webster J, Liu Z, Norman G, et al. Negative pressure wound therapy for surgical wounds healing by primary closure. Cochrane Database Syst Rev. 2019;3(3):CD009261. doi:10.1002/14651858.CD009261.pub4
45. Singh DP, Gabriel A, Parvizi J, Gardner MJ, D'Agostino R Jr. Meta-analysis of comparative trials evaluating a single-use closed-incision negative-pressure therapy system. Plast Reconstr Surg. 2019;143(1S Management of Surgical Incisions Utilizing Closed-Incision Negative-Pressure Therapy):41S-46S. doi:10.1097/PRS.0000000000005312
46. Mir A, Guys N, Arianpour K, et al. Negative pressure wound therapy in the head and neck: an evidence-based approach. Laryngoscope. 2019;129(3):671-683. doi:10.1002/lary.27262
47. Svensson-Björk R, Zarrouk M, Asciutto G, Hasselmann J, Acosta S. Meta-analysis of negative pressure wound therapy of closed groin incisions in arterial surgery. Br J Surg. 2019;106(4):310-318. doi:10.1002/bjs.11100
48. Wynn M, Freeman S. The efficacy of negative pressure wound therapy for diabetic foot ulcers: A systematised review. J Tissue Viability. 2019;28(3):152-160. doi:10.1016/j.jtv.2019.04.001
49. Ge D. The safety of negative-pressure wound therapy on surgical wounds. Adv Skin Wound Care. 2018;31(9):421-428. doi:10.1097/01.ASW.0000542530.71686.5c
50. Li L, Liu W, Tao H, et al. Efficacy and safety of negative pressure versus natural drainage after thyroid surgery. Medicine. 2018;97(31):e11576. doi:10.1097/MD.0000000000011576
51. Iheozor-Ejiofor Z, Newton K, Dumville JC, Costa ML, Norman G, Bruce J. Negative pressure wound therapy for open traumatic wounds. Cochrane Database Syst Rev. 2018;7(7):CD012522. doi:10.1002/14651858.CD012522.pub2
52. Liu X, Zhang H, Cen S, Huang F. Negative pressure wound therapy versus conventional wound dressings in treatment of open fractures: a systematic review and meta-analysis. Int J Surg. 2018;53:72-79. doi:10.1016/j.ijsu.2018.02.064
53. Hyldig N, Birke-Sorensen H, Kruse M, et al. Meta-analysis of negative-pressure wound therapy for closed surgical incisions. Br J Surg. 2016;103(5):477-486. doi:10.1002/bjs.10084






