Pancreatitis Caused by Campylobacter Enteritis
A 30-year-old man presented to the emergency department with upper abdominal pain radiating to the back.
History and physical examination. The onset of pain was approximately 4 to 5 days before, and he rated it as 8 of 10 in intensity. The pain was associated with diarrhea, including 1 episode of hematochezia. He denied nausea, vomiting, or any other symptoms. He denied any medical conditions or past surgical procedures. His social history was positive for occasional alcohol consumption (1-2 beers), but he denied tobacco or drug use. Epigastric tenderness was present on physical examination. His vital signs were stable at presentation, with normal temperature.
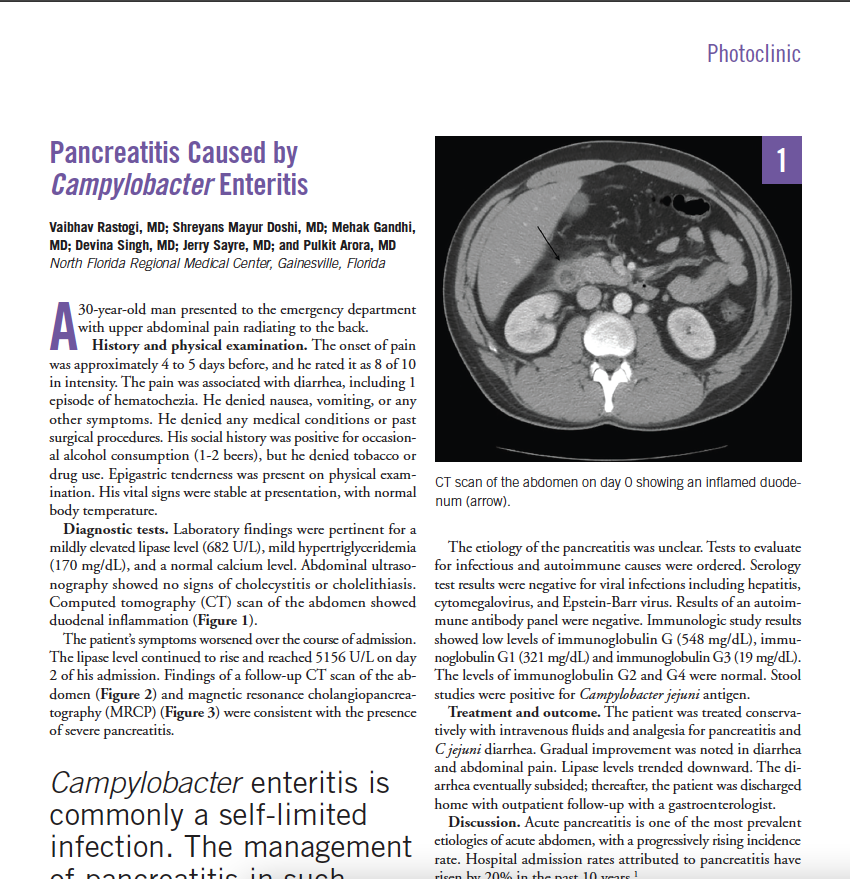
Diagnostic tests. Laboratory findings were pertinent for a mildly elevated lipase level (682 U/L), mild hypertriglyceridemia (170 mg/dL), and a normal calcium level. Abdominal ultrasonography showed no signs of cholecystitis or cholelithiasis. Computed tomography (CT) scan of the abdomen showed duodenal inflammation (Figure 1).
The patient’s symptoms worsened over the course of admission. The lipase level continued to rise and reached 5156 U/L on day 2 of admission. Findings of a follow-up CT scan of the abdomen (Figure 2) and magnetic resonance cholangiopancreatography (MRCP) (Figure 3) were consistent with the presence of severe pancreatitis.
The etiology of the pancreatitis was unclear. Tests to evaluate for infectious and autoimmune causes were ordered. Serology test results were negative for viral infections including hepatitis, cytomegalovirus, and Epstein-Barr virus. Results of an autoimmune antibody panel were negative. Immunologic study results showed low levels of immunoglobulin G (548 mg/dL), immunoglobulin G1 (321 mg/dL) and immunoglobulin G3 (19 mg/dL). The levels of immunoglobulin G2 and G4 were normal. Stool studies were positive for Campylobacter jejuni antigen.
Treatment and outcome. The patient was treated conservatively with intravenous fluids and analgesia for pancreatitis and C jejuni diarrhea. Gradual improvement was noted in diarrhea and abdominal pain. Lipase levels trended downward. The diarrhea eventually subsided; thereafter, the patient was discharged home with outpatient follow-up with a gastroenterologist.
Discussion. Acute pancreatitis is one of the most prevalent etiologies of acute abdomen, with a progressively rising incidence rate. Hospital admission rates attributed to pancreatitis have risen by 20% in the past 10 years.1 The most common etiologies include gallstones (approximately 40% of cases) and alcohol use (approximately 30% of cases). Other cases of acute pancreatitis are idiopathic or related to hypertriglyceridemia, drug use, trauma, or endoscopic retrograde cholangiopancreatography.1
Infections rarely precipitate pancreatitis. Viruses such as mumps virus, coxsackievirus, hepatitis B virus, cytomegalovirus, varicella-zoster virus, herpes simplex virus, and HIV have been reported to cause pancreatitis.2 Bacteria associated with pancreatitis include Mycoplasma, Legionella, Salmonella enterica subsp enterica ser Typhi, Leptospira, Campylobacter, Yersinia enterocolitica, and Yersinia pseudotuberculosis.2,3 Certain fungi and parasites also have been linked to pancreatitis.2
This article includes supplementary material, which can be accessed here
Infection with Campylobacter, a gram-negative bacteria, is one of the most common etiologies for diarrheal illness in the United States. C jejuni and Campylobacter coli are mainly responsible for diseases in humans. The transmission usually occurs through contaminated food (especially meat) and water.4 It is well known for causing bloody or watery diarrhea. However, extraintestinal manifestations or disorders such as endocarditis, glomerulonephritis, meningitis, and pancreatitis can also be seen as a consequence of Campylobacter infection.5
The exact pathogenesis of Campylobacter-induced pancreatitis is unknown. Multiple theories have been postulated for the bacterial causation of pancreatitis. These include translocation of the bacteria from the gut to the pancreas or direct spread from any other surrounding organ.3 They can also spread through the blood vessels and lymphatics or can directly intrude the bile duct or pancreatic duct.2 Autoimmune-mediated pancreatitis as a result of host immune response to the offending pathogen might also be a cause.3
Prior studies have shown the association of pancreatitis with Campylobacter infection.3,5,6 Pitkänen and colleagues5 retrospectively analyzed data from 188 hospitalized patients with Campylobacter enteritis. They found that 11 patients had pancreatitis. The age of occurrence varies widely, and there is no gender-based difference. The development of pancreatitis is seen 3 to 7 days after the enteritis presentation.3
A true causal relationship between Campylobacter enteritis and pancreatitis has not yet been established. Campylobacter is considered the causative entity if other factors causing pancreatitis have been ruled out and concomitant Campylobacter infection is present. In our patient’s case, we ruled out other factors (occasional alcohol intake, no smoking, no gallstones, mild hypertriglyceridemia, normal autoantibody titers, normal or low immunoglobulin G levels, normal serum calcium, no trauma, no home medications, and no anatomic abnormalities in the pancreas) to diagnose Campylobacter enteritis as the source of pancreatitis (Supplemental table 1).
Campylobacter enteritis is commonly a self-limited infection.4 The management of pancreatitis in such cases depends on the underlying gastroenteritis and usually is supportive therapy, including intravenous fluids, electrolyte management, and bowel rest.3 Antibiotics can be used if the patient is not improving with supportive therapy or if severe disease develops. In our patient, piperacillin-tazobactam was started for pneumonia, which might have also covered Campylobacter infection.
References:
1. Forsmark CE, Vege SS, Wilcox CM. Acute Pancreatitis. N Engl J Med. 2016;375(20):1972-1981.
2. Parenti DM, Steinberg W, Kang P. Infectious causes of acute pancreatitis. Pancreas. 1996;13(4):356-371.
3. Kobayashi R, Matsumoto S, Yoshida Y. Case of acute pancreatitis associated with Campylobacter enteritis. World J Gastroenterol. 2014;20(23):7514-7517.
4. Dasti JI, Tareen AM, Lugert R, Zautner AE, Gross U. Campylobacter jejuni: a brief overview on pathogenicity-associated factors and disease-mediating mechanisms. Int J Med Microbiol. 2010;300(4):205-211.
5. Pitkänen T, Pönkä A, Pettersson T, Kosunen TU. Campylobacter enteritis in 188 hospitalized patients. Arch Intern Med. 1983;143(2):215-219.
6. Ezpeleta C, de Ursua PR, Obregon F, Goñi F, Cisterna R. Acute pancreatitis associated with Campylobacter jejuni bacteremia. Clin Infect Dis. 1992;15(6):1050.
Figure 1. CT scan of the abdomen on day 0 showing an inflamed duodenum (arrow).
Figure 2. CT scan of the abdomen on day 3 showing moderate to severe peripancreatic inflammatory changes, mainly affecting body and tail of pancreas (arrows).
Figure 3. MRCP showing increased peripancreatic fluid consistent with progressed severe pancreatitis. No choledocholithiasis, biliary stricture, or biliary duct dilation were noted.