

Arterial Discordance in Cardiac Tamponade
Abstract: Ventricular interdependence is a salient hemodynamic feature of cardiac tamponade that manifests as discordance between the left and right ventricles in filling and ejection on hemodynamic assessment. Ventricular interdependence can manifest as arterial discordance at the level of the great arteries.
J INVASIVE CARDIOL 2016;28(10):E124-E125
Key words: Cardiac tamponade, ventricular interdependence, pericardiocentesis, pericardial effusion
Case Presentation
A 62-year-old woman with squamous cell carcinoma of the right lung presented with subacute breathlessness for 1 week. She was tachypneic at rest and the jugular venous pressure was elevated with absent “y” descent. Pulsus paradoxus of 40 mm Hg was documented and the heart sounds were muffled. Lung bases were clear. Electrocardiogram revealed sinus tachycardia with low-voltage complexes and electrical alternans. Two-dimensional transthoracic echocardiogram showed large circumferential pericardial effusion with diastolic collapse of the right ventricular outflow tract and 50% respiratory variation in tricuspid inflow velocities suggestive of cardiac tamponade. An emergency pericardiocentesis was done with good result.
The hemodynamic studies at baseline and post pericardiocentesis demonstrated interesting findings, ie, equalization of the ventricular diastolic and intrapericardial pressures consistent with tamponade physiology. Simultaneous pressure tracing showed ventricular interdependence with discordant relationship of the left and right ventricles. Interestingly, a simultaneous main pulmonary artery and ascending aortic pressure recording showed similar discordant relationship of pressures in the great arteries (Figure 1). While the systolic pulmonary artery pressure increased at inspiration, this was accompanied by a fall in systolic ascending aortic pressure. The converse was noted in expiration, suggesting arterial discordance.
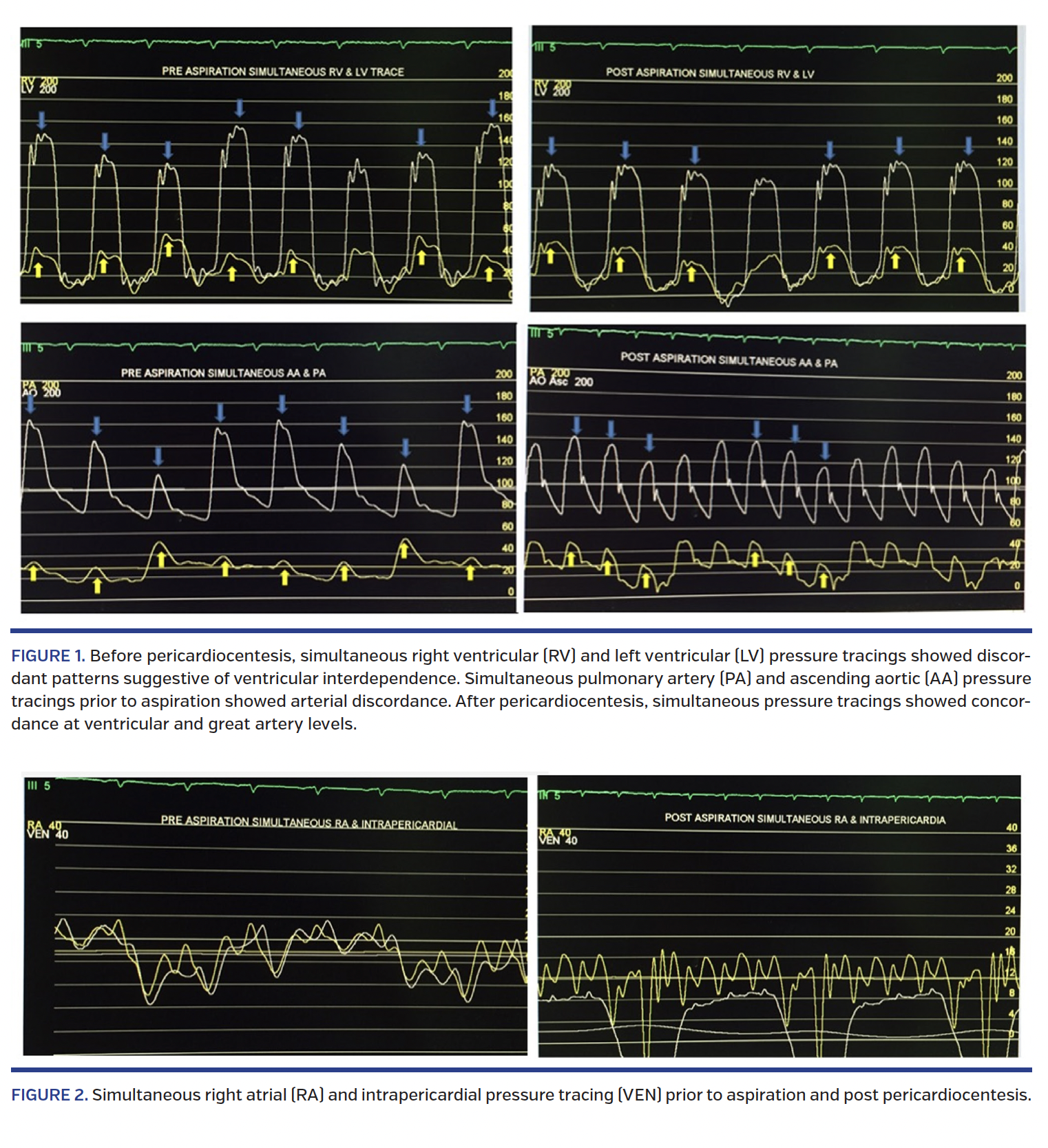
Pericardiocentesis produced 450 mL of hemorrhagic fluid and restored the mean intrapericardial pressure to 0 mm Hg. Pericardiocentesis resulted in reappearance of the “y” descent (Figure 2). The right atrial mean pressure remained elevated, although the intrapericardial pressures were restored to 0 mm Hg. Neither diastolic pressure equalization nor ventricular or arterial discordance could be demonstrated post pericardiocentesis.
Discussion
Cardiac tamponade is characterized by restrictive ventricular filling that varies with respiration. The right atrial pressure is significantly elevated with absent “y” descent. The respiratory variation has differential effect on right and left ventricular filling and ejection and forms the basis of hemodynamic changes. It is manifested as ventricular interdependence, in which filling of one ventricle is out of phase with the other ventricle. Ventricular interdependence, a salient hemodynamic feature of cardiac tamponade, is usually observed as ventricular discordance where filling of either ventricle occurs out of phase with the other.1,2 Reduced left ventricular filling during inspiration allows a shift of the interventricular septum to the left, causing an increase in filling and output from the right ventricle during inspiration and vice versa. Ventricular discordance could reflect as discordance in the great artery pressure tracings provided the pulmonary and aortic valves are competent.
References
1. Shaver JA, Reddy PS, Curtiss EI, Ziady GM, Reddy SC. Non-invasive/invasive correlates of exaggerated ventricular interdependence in cardiac tamponade. J Cardiol. 2001;37(Suppl 1):71-76.
2. Santamore WP, Dell’Italia LJ. Ventricular interdependence: significant left ventricular contributions to right ventricular systolic function. Prog Cardiovasc Dis. 1998;40:289-308.
From the Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 16, 2016 and accepted May 31, 2016.
Address for correspondence: Dr Arun Gopalakrishnan, Department of Cardiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Thiruvananthapuram, Kerala, India – 695011. Email: arungopalakrishnan99@gmail.com









