

Isolated Single Coronary Artery Arising from the Right Sinus of Valsalva
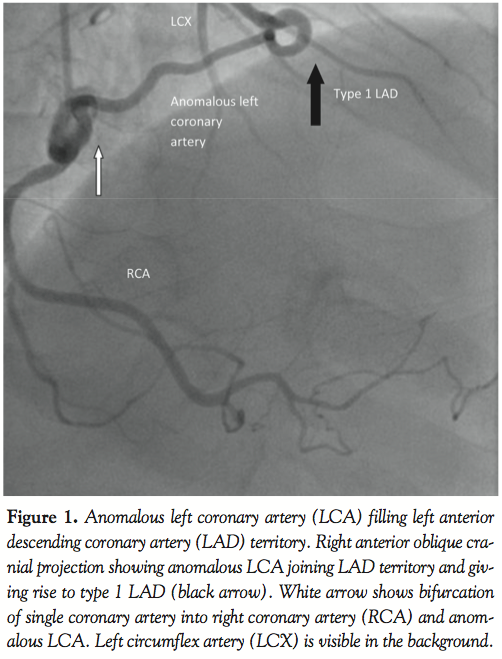
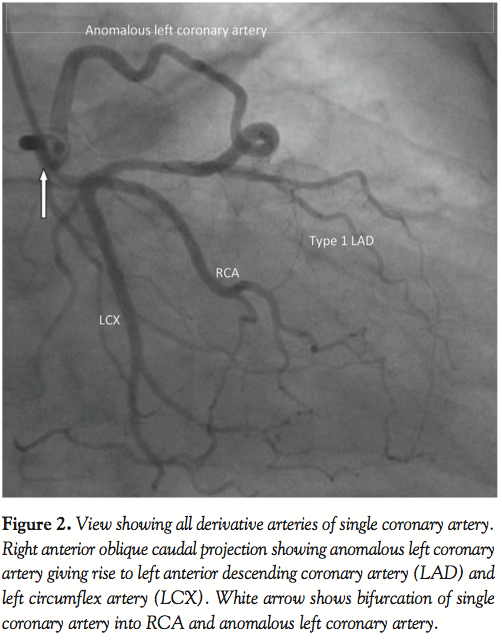
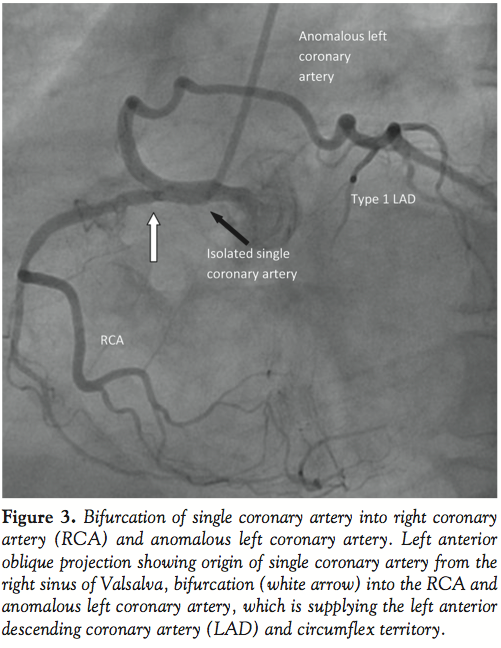
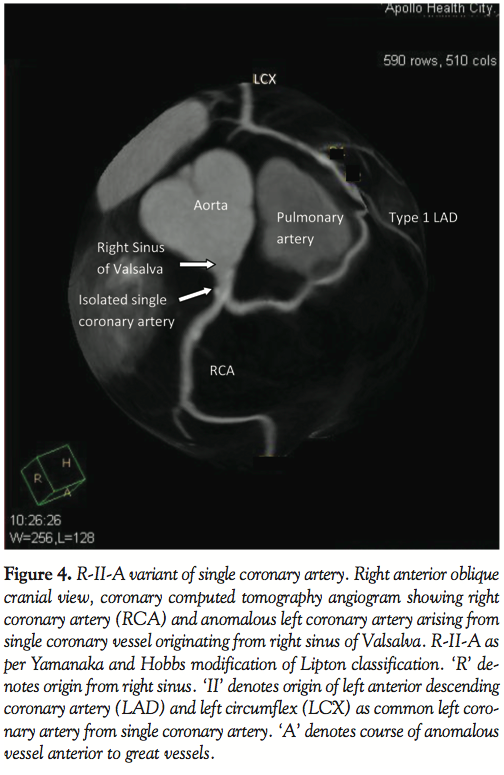
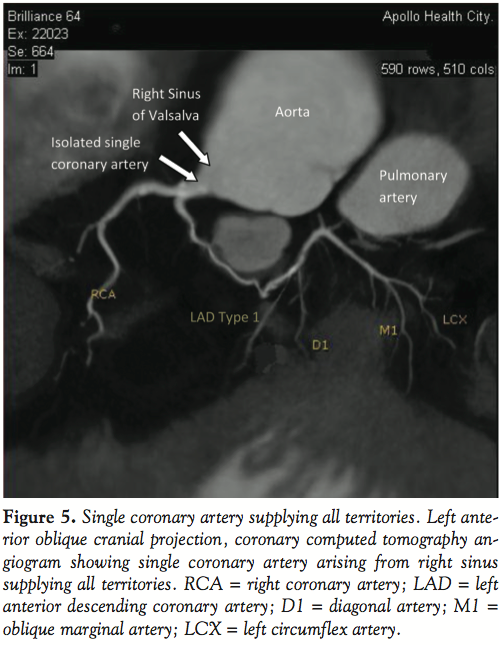
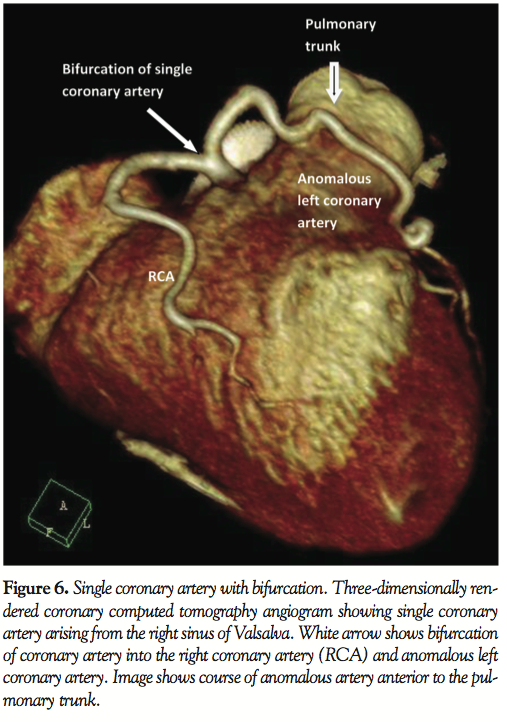
A 59-year-old man with a history of hypertension, family history of premature coronary artery disease and atypical chest heaviness was referred to exercise stress test. After achieving 89% target heart rate at a workload of 9 metabolic equivalents using Bruce protocol, 1–1.5 mm horizontal ST depressions were seen in the lateral leads. Coronary angiogram revealed a single coronary artery originating from the right sinus of Valsalva; this artery bifurcated into a right coronary artery and an anomalous left main coronary artery. Multi-detector row computed tomography confirmed the same findings. The anomalous left coronary artery followed a pre-pulmonary course anterior to the pulmonary trunk to supply the anterior descending, diagonals and circumflex artery. There was no evidence of an inter-arterial course, which is considered malignant. The coronary arteries were free of atherosclerotic disease. Stress myocardial perfusion imaging showed no inducible ischemia. Echocardiogram showed normal left ventricular function.
The overall incidence of single coronary artery disease in a series of consecutive angiograms is between 0.024%1 and 0.044%.2 An aberrant left main artery arising from a single coronary artery from the right sinus of Valsalva (R-II-A as per modified Lipton classification) was seen in 4 cases out of a series of 50,000 angiograms.3
Prognosis of individuals with single coronary artery is uncertain, with no established treatment guidelines. In general, anomalies with right-sided origin and a pre-pulmonary course are considered harmless.4 Revascularization would be considered only with atherosclerotic changes and documented ischemia.
Acknowledgment: The funding for coronary imaging was provided by Apollo Health City, Jubilee Hills. We also gratefully acknowledge the considerable support provided by Dr. Hariprasad, CEO, Apollo Health City and Dr. Jyotsna Rao, Consultant, Department of Nuclear Medicine and PET-CT Centre, Apollo Health City, Hyderabad, India.

JIC-IC-11-00007-sd01-Single_coronary_artery_video.avi
References
- Lipton MJ, Bany WH, Obrez I, Silverrnan JF, Wexler L: Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology 1979;130:39-47.
- Yamanaka O, Hobbs RE. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn 1990;21:29–40.
- Desmet W, Vanhaecke J, Vrolix M, et al. Isolated single coronary artery: A review of 50,000 consecutive coronary angiographies. Eur Heart J 1992;13:1637–1640.
- Basso C, Maron BJ, Corrado D, Thiene G. Clinical role of congenital coronary artery anomalies with origin from the wrong aortic sinus leading to sudden death in young competitive athletes.J Am Coll Cardiol 2000;35:1493–1501.
_____________________________________
*Joint first authors.
From the 1Department of Cardiology, 2Department of Clinical Research, and 3Department of Radiology, Apollo Health City, Jubilee Hills, Hyderabad, India.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted January 12, 2011, provisional acceptance given January 24, 2011, final version accepted January 26, 2011.
Address for correspondence: Auras Ravi Atreya, MD, Center for Arrhythmia Research, University of Michigan, 5025 Venture Drive, Ann Arbor, MI 48108-0372. Email: auras@umich.edu












