Planned Robotic Chronic Total Occlusion Percutaneous Coronary Intervention: Feasibility Report
Abstract: Background. Complex robotic percutaneous coronary intervention (R-PCI) is technically possible and leads to clinically comparable outcomes compared with the manual approach. However, there are limited data on the feasibility of chronic total occlusion (CTO) revascularization via the R-PCI approach. Methods. Ten consecutive patients undergoing R-PCI for a coronary CTO at a single tertiary academic center were analyzed. The PRECISION, PRECISION GRX, and PROGRESS CTO registries were utilized for data collection with regard to procedural/clinical details and results. Results. Technical success, defined as successful CTO revascularization with full or partial robotic support, occurred in 7 of 10 patients. There were no periprocedural major adverse cardiac events. Average J-CTO score was 2; all procedures were performed from an antegrade approach. The time from robotic wire manipulation to completion of procedure regardless of method averaged 55.1 minutes; average fluoroscopy time was 29.9 minutes. Conclusions. CTO revascularization via a robotic approach is feasible. Technical success may be best predicted by those patients with low J-CTO scores and lesions amenable to antegrade wire escalation technique. Given the potential benefits to both operators and patients, further research is warranted.
Key words: chronic total occlusion, robotic PCI
The performance of percutaneous coronary intervention (PCI) is fraught with occupational hazards for the operating physician. Despite clinical advances throughout over 40 years of interventional cardiology, the procedure itself has been largely unchanged: an operator stands bedside next to a patient, manually manipulating interventional equipment under fluoroscopic guidance. Ionizing radiation produced by fluoroscopy causes significant harm to the operator, including increasing the risk of a malignancy and cataract formation.1,2 Furthermore, nearly half of all operators report an orthopedic injury incurred by the necessary precaution of wearing heavy lead aprons to protect from this ionizing radiation.3 Robotic PCI (R-PCI) with the CorPath System (Corindus) moves the operator from bedside and into a cockpit where they can manipulate equipment remotely while protected by lead shielding. This eliminates the risk of radiation exposure and obviates the need for lead aprons. R-PCI is both safe and effective in simple and complex coronary lesions, with durable long-term clinical outcomes,4-6 and represents an important innovation for operator protection.
One of the most significant and rapidly growing areas in the field of interventional cardiology is the percutaneous treatment of chronic total occlusion (CTO) lesions. They are highly prevalent; in those patients undergoing diagnostic angiography, approximately 30% will have a CTO.7,8 This increases to over 50% in patients who have previously undergone coronary artery bypass graft surgery.9 CTO revascularization improves symptoms in those patients with stable ischemic heart disease10 and CTO revascularization, in particular of the left anterior descending artery, may improve systolic function and offer improved long-term survival.11,12 R-PCI for the treatment of CTOs is an attractive option, as CTO-PCI has overall radiation exposure doses that are four times higher than standard PCI.13 By placing the operator in a leaded cockpit away from the procedural table, direct exposure to radiation is removed and the prolonged need for wearing lead is eliminated. However, thus far there have been no data demonstrating complete R-PCI for coronary CTO lesions. We undertook this study to determine the feasibility of R-PCI for treating coronary CTO lesions.
Methods
Study population. This single-center study at a tertiary academic center included patients who had undergone R-PCI for coronary CTO lesions as a part of ongoing robotic registry studies. The definition of CTO has been previously published.14 All consecutive R-PCI CTO interventions performed utilizing the CorPath 200 robotic-assisted PCI system or the new-generation CorPath GRX system were included.
Data collection. Data were collected from the following registries: PRECISION (Post-market CorPath Registry on the CorPath 200 System in Percutaneous Coronary Intervention; NCT01917682); PRECISION GRX (NCT03278301); and PROGRESS-CTO (Prospective Global Registry for the Study of Chronic Total Occlusions; NCT02061436). Demographics, lesion characteristics, and interventional details were assessed in all patients.
Definitions. R-PCI technical success was defined as successful CTO revascularization either completely robotically or with partial manual assistance. R-PCI clinical success was defined as technical success without in-hospital major adverse cardiac events (MACE; defined as death, stroke, myocardial infarction, or urgent revascularization).
Results
Ten patients (8 men and 2 women; mean age, 69.1 ± 6.7 years) underwent planned R-PCI for CTO revascularization. There was a high prevalence of typical coronary artery disease risk factors within the cohort. Two patients had chronic kidney disease, and 2 patients had mild systolic dysfunction (Table 1). The majority of CTO lesions treated were in the right coronary artery (60%) and the average occlusion length was 29.2 mm. Average J-CTO score was 2, PROGRESS CTO score was 1.4, and PROGRESS CTO Complications score was 3.3 (Table 2).
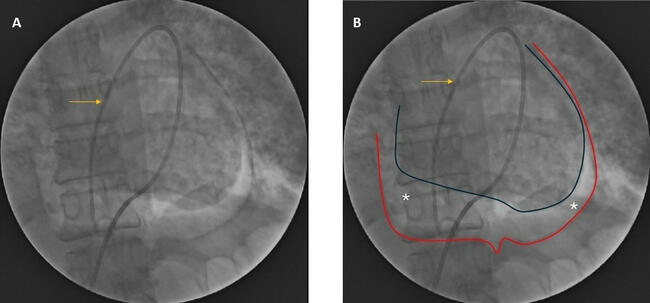
An antegrade wire escalation approach was utilized in each case as the initial crossing technique. CTO revascularization was successful in 9 of the 10 cases. Technical success and clinical success were achieved in 7 of the 10 cases (Figure 1). Complete robotic intervention with no need for any manual guide, balloon, or wire manipulation was possible in 6 of the 10 cases. Total robotic procedural time, defined as time from robotic wire manipulation to completion of procedure regardless of method, averaged 55.1 ± 28.7 minutes, with mean fluoroscopy time of 29.9 ± 14.5 minutes and contrast use of 223 ± 66.3 mL. Of the 4 procedures requiring manual PCI, one required partial manual assistance for guide manipulation. The other 3 procedures resulted in complete conversion to a manual approach due to unplanned bifurcation intervention, acute vessel closure requiring urgent management, and inadequate guide-catheter support. There were no MACE within the cohort (Table 3).
Discussion
This is the first description of an attempt at complete robotic CTO revascularization. In the presented series, overall there was a 90% success in CTO intervention; this is in line with the highest reported rate of successful CTO-PCI at high-volume centers that report outcomes to national multicenter CTO registries.15,16 Contrast use, fluoroscopy time, and overall procedural time are also comparable with these reports. The success rate for complete robotic CTO-PCI was 60%; of the 4 patients unable to have successful complete robotic intervention, one underwent completion of the procedure robotically after the guide was adjusted manually. Two patients had successful procedure completion after complete manual conversion, and as noted above, one patient did not have a successful CTO revascularization. Notably, the patient requiring partial manual assistance had the procedure performed utilizing the now outdated CorPath 200 system; the new-generation CorPath GRX system allows for robotic guide manipulation. This patient series demonstrates that robotic CTO revascularization is feasible and safe in a series of selected CTO procedures that were all attempted via the antegrade wire escalation technique.
It is notable that all procedures reported in this initial feasibility report were performed utilizing an antegrade wire escalation approach as the initial crossing method. While the hybrid algorithm does advocate this as a standard first choice, in particular with less complex lesions, the robotic platform is limited to only this approach. The robotic platform is strictly a rapid-exchange instrument, and therefore a wire can only be advanced along with a rapid-exchange balloon for support. Common CTO antegrade approach requires the use of microcatheters and often frequent guidewire exchanges, which is more difficult to do with the robotic platform as it entails losing the distal guidewire positioning. The position of a second wire port on the robotic instrument does allow for a parallel wire or see-saw procedure; however, more complex crossing techniques such as dissection re-entry or retrograde revascularization require manual crossing of the lesion prior to robotic connection for procedure completion. This so-called “hybrid” robotic technique has recently been described.17 Finally, this was a non-randomized, observational study assessing safety and feasibility of a completely R-PCI CTO procedure; although J-CTO and PROGRESS CTO scores were on average moderately difficult, only 2 of the patients had greater than mild/moderate calcification, and no patient had a J-CTO or PROGRESS CTO score higher than 3. As such, complete robotic CTO revascularization as demonstrated may be suitable as an isolated technique in those patients felt to be at highest potential for successful antegrade wire escalation.
Conclusions
CTO revascularization via a robotic approach is feasible in select lesions and patients. Technical success may be best predicted by those patients with low J-CTO scores and lesions amenable to aggressive antegrade wire escalation technique. Given the potential benefits to both operators and patients, further research is warranted.
From the University of California, San Diego, La Jolla, California.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Mahmud reports grant support from Corindus, manufacturer of the robotic platform used in this study, and is the national PI for the PRECISION GRX study. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted January 17, 2020, final version accepted January 29, 2020.
Address for correspondence: Ehtisham Mahmud, MD, FACC, FSCAI, Sulpizio Cardiovascular Center, 9434 Medical Center Drive, La Jolla, CA 92037. Email: emahmud@ucsd.edu
- Vano E, Kleiman NJ, Duran A, Rehani MM, Echeverri D, Cabrera M. Radiation cataract risk in interventional cardiology personnel. Radiat Res. 2010;174:490-495.
- Eisenberg MJ, Afilalo J, Lawler PR, Abrahamowicz M, Richard H, Pilote LMMP. Cancer risk related to low-dose ionizing radiation from cardiac imaging in patients after acute myocardial infarction. CMAJ. 2011;183:430-436.
- Klein LW, Tra Y, Garratt KN, et al. Society for Cardiovascular Angiography and Interventions. Occupational health hazards of interventional cardiologists in the current decade: results of the 2014 SCAI membership survey. Catheter Cardiovasc Interv. 2015;86:913-924.
- Weisz G, Metzger DC, Caputo RP, et al. Safety and feasibility of robotic percutaneous coronary intervention: PRECISE (Percutaneous RoboticallyEnhanced Coronary Intervention) study. J Am Coll Cardiol. 2013;61:1596-1600.
- Mahmud E, Naghi J, Ang L, et al. Demonstration of the safety and feasibility of robotically assisted percutaneous coronary intervention in complex coronary lesions: results of the CORA-PCI study (Complex Robotically Assisted Percutaneous Coronary Intervention). JACC Cardiovasc Interv. 2017;10:1320-1327.
- Walters DC, Reeves RR, Patel MP, et al. Complex robotic compared to manual coronary interventions: 6- and 12-month outcomes. Catheter Cardiovasc Interv. 2019;93:613-617. Epub 2018 Nov 19.
- Jeroudi OM, Alomar ME, Michael TT, et al. Prevalence and management of coronary chronic total occlusions in a tertiary Veterans Affairs hospital. Catheter Cardiovasc Interv. 2014;84:637. Epub 2013 Nov 13.
- Tsai TT, Stanislawski MA, Shunk KA, et al. Contemporary incidence, management, and long-term outcomes of percutaneous coronary interventions for chronic coronary artery total occlusions: insights from the VA CART program. JACC Cardiovasc Interv. 2017;10:866.
- Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59:991.
- Joyal D, Afilalo J, Rinfret S. Effectiveness of recanalization of chronic total occlusions: a systematic review and meta-analysis. Am Heart J. 2010;160:179-187.
- Henriques JP, Hoebers LP, Råmunddal T, et al. Percutaneous intervention for concurrent chronic total occlusions in patients with STEMI: the EXPLORE trial. J Am Coll Cardiol. 2016;68:1622-1632.
- Safley DM, House JA, Marso SP, Grantham JA, Rutherford BD. Improvement in survival following successful percutaneous coronary intervention of coronary chronic total occlusions: variability by target vessel. JACC Cardiovasc Interv. 2008;1:295-302.
- Pavlidis AN, Jones DA, Sirker A, Mathur A, Smith EJ. Reducing radiation in chronic total occlusion percutaneous coronary interventions. Curr Cardiol Rev. 2016;12:12-17.
- Stone GW, Kandzari DE, Mehran R, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part I. Circulation. 2005;112:2364.
- Habara M, Tsuchikane E, Muramatsu T, et al; Retrograde Summit Investigators. Comparison of percutaneous coronary intervention for chronic total occlusion outcome according to operator experience from the Japanese retrograde summit registry. Catheter Cardiovasc Interv. 2016;87:1027-1035.
- Christopoulos G, Karmpaliotis D, Alaswad K, et al. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228.
- Hirai T, Kearney K, Kataruka A, et al. Initial report of safety and procedure duration of robotic-assisted chronic total occlusion coronary intervention. Catheter Cardiovasc Interv. 2020;95:165-169. Epub 2019 Sep 4.