

Vascular Assessment for Transcatheter Aortic Valve Replacement: Intravascular Ultrasound Compared With Computed Tomography
Abstract: Background. Assessment of the femoral and iliac arteries is essential prior to transcatheter aortic valve replacement (TAVR). It is critical for establishing candidacy for a femoral approach, and can help predict vascular complications. Although computed tomography angiography (CTA) is the standard imaging modality, it has limitations. Objective. This study compared CTA with intravascular ultrasound (IVUS) in patients undergoing TAVR evaluation. Methods. Fifteen patients undergoing pre-TAVR coronary angiography and hemodynamic assessment were recruited. Following coronary angiography, patients underwent distal aortography, bilateral iliac and femoral arteriography, and IVUS assessment. Vascular tortuosity, minimum lumen diameter, and cross-sectional area were obtained and the findings were compared with those obtained from CTA. Results. Correlation between IVUS and CTA was strong for minimum luminal diameter (r=0.62). Concordance was also strong between CTA and invasive iliofemoral angiography for assessment of tortuosity (r=0.75). Utilizing Bland-Altman analysis, vessel diameters obtained by IVUS were consistently greater than those obtained by CTA. The angiography and IVUS strategy was associated with a lower overall mean contrast utilization (29 cc vs 100 cc; P<.001), reduced mean radiation exposure (527 mGy vs 998 mGy; P=.045), and no significant difference in mean test duration (13.3 minutes vs 10 minutes; P=.12). Conclusions. For femoral and iliac arterial assessment prior to TAVR, IVUS is a viable alternative to CTA with comparable accuracy, and the potential for less contrast use and less radiation exposure. IVUS is also a valuable adjunct to CTA in patients with borderline femoral access diameters or considerable CTA artifacts.
J INVASIVE CARDIOL 2016;28(12):E172-E178.
Key words: aortic valve replacement, vascular complications
Aortic valve replacement (AVR) improves symptoms and prolongs life in patients with symptomatic severe aortic stenosis (AS).1 Transcatheter aortic valve replacement (TAVR) is currently employed as an alternative to surgery, and shows at least comparable outcomes in intermediate and high-risk surgical candidates.2-4 Although femoral artery access is preferred for TAVR, the vascular complication rate ranges from 6.3%-30.7%.5-7At times, the diameter of valve-delivery sheath exceeds the femoral and/or iliac artery diameter, leading to vascular complications or decision to utilize an alternative access, both of which are associated with worse outcomes.5 A careful assessment of the femoral and iliac arteries before TAVR is therefore crucial and involves an adequate assessment of arterial size, tortuosity, and degree of calcification.
Multidetector computed tomography angiography (CTA) has been the standard modality employed for this purpose. However, there are safety and cost considerations related to the amount of radiation used, the necessity of high load of intravenous contrast, and the effort involved in three-dimensional (3D) reconstructions.8 In addition, blooming artifacts can occur due to the presence of intense calcification or indwelling stents. These artifacts can compromise image quality and interfere with interpretation.
The use of intravascular ultrasound (IVUS) for access planning has the potential to reduce overall contrast use, decrease radiation, and increase the precision of femoral and iliac artery assessment.9 Although peripheral IVUS is occasionally performed in cases of equivocal CTA results, this strategy has not been directly compared with CTA. Previous studies have demonstrated good correlation between coronary CTA and coronary IVUS,10,11 but this is not well studied in peripheral IVUS. This study aims to assess the accuracy and safety of pre-TAVR femoral and iliac artery assessment by IVUS when compared with CTA.
Methods
Patient selection. The study design was prospective observational from March 2014 to March 2015. Patients referred for TAVR were recruited for participation at the time of coronary angiography and hemodynamic assessment in the catheterization laboratory. Patients were excluded if they had known occlusion of the common iliac, external iliac, or common femoral artery, or if they had critical limb ischemia. Baseline demographics, medical comorbidities, clinical presentation, and current medications were recorded. This project was approved by Ohio State University’s Institutional Review Board and subjects gave informed consent prior to enrollment.
Instrumentation and data acquisition. Study patients underwent routine TAVR work-up including CTA of the aorta, iliac, and femoral arteries, which was interpreted by a radiologist independent of the study per usual protocol. At the time of the coronary angiography, each study patient underwent distal aorta, bilateral iliac and femoral run-off angiography, and assessment of the right and left iliac and common femoral arteries with peripheral IVUS (Eagle Eye Platinum IVUS catheter; Volcano Corporation).
If access for coronary angiogram was obtained via the femoral artery, a 5 Fr or 6 Fr internal mammary artery (IMA) guiding catheter was advanced to the iliac bifurcation and a 0.014˝ Mailman coronary wire (Boston Scientific) was advanced down the contralateral iliac artery to the common femoral artery. Next, the IVUS catheter was advanced over the Mailman wire to the contralateral common femoral artery. Data obtained during a slow pull-back of the IVUS catheter were recorded on the Volcano imaging software. Once the contralateral vessel (common femoral to aortic bifurcation) images were collected, the Mailman wire was retracted and extended into the distal aorta. Ipsilateral common iliac artery to common femoral artery IVUS was performed next. If needed, the existing sheath was slightly retracted to image the common femoral artery near the arteriotomy site. If access was obtained in the radial artery, a 5 Fr or 6 Fr IMA or Judkins right (JR) guiding catheter and a 300 cm, 0.035˝ Mailman was advanced to the common femoral artery on one side. The IVUS catheter was advanced over this wire, and images were collected. Then, the wire and IVUS catheter were pulled back to the distal aorta and the wire passed into the contralateral iliac system, with imaging from common femoral to aortic bifurcation as described. After collection of the images, hemostasis was obtained in the standard manner per operator’s usual practice.
IVUS images were reconstructed utilizing the Volcano IVUS imaging software. Lumen, media, and adventitial contours were manually defined for each gray-scale image, and verified by an independent operator. Data were reviewed and graded by an interventional cardiologist experienced in IVUS interpretation and blinded to the CTA results. The distal aortogram and bilateral iliofemoral angiogram were also used to assess the tortuosity of the vasculature. Tortuosity was classified as follows: mild (30° to 60° bend); moderate (60° to 90° bend); or severe (>90° bend), as described elsewhere.12
Baseline demographics and clinical characteristics were recorded, and procedural variables were collected during and after the TAVR procedure.
Statistical analyses. Patient variables are expressed as proportions for dichotomous variables and mean ± standard deviation for continuous variables. Differences between CTA and IVUS were determined by the paired Student’s t-test for parametric data such as contrast utilization, radiation utilization, and duration of test. In order to assess inter-rater concordance and agreement between CTA and IVUS regarding minimum luminal diameter measurement, Bland-Altman analysis was used for both vessel and vessel segments in addition to Pearson’s correlation. We chose Bland-Altman as the primary statistical approach for comparison because it allows quantification of the agreement between IVUS and CTA by studying the mean difference and constructing limits of agreement.13,14 Furthermore, it helps evaluate the bias between the mean differences, and helps estimate an agreement interval, within which 95% of the differences of the second method, compared with the first one.13 Using both Pearson and Bland-Altman methods allows more accurate comparison of the inter-rater agreement between CTA and IVUS. Statistical significance was set at P<.05. All analyses were performed utilizing SPSS 16.0 (SPSS, Inc). We elected to analyze size comparisons in two ways: (1) to determine how the IVUS and CTA results correlated; and (2) to determine whether IVUS-measured vessel diameters were consistently greater or less than values derived from CTA.
We analyzed the vasculature from each participant in a “per segment” (common femoral, external iliac, common iliac) and “per-vessel” (right or left iliofemoral vessel) manner. The correlation between iliofemoral artery size with IVUS and CTA was evaluated utilizing linear regression with calculation of Pearson correlation coefficients. Arterial diameters used in the comparison were the minimum luminal diameters obtained by IVUS and CTA.
Vessel tortuosity was evaluated by two interventional cardiologists blinded to the CTA results. Similarly, tortuosity was evaluated on CTA by a radiologist blinded to the invasive aortography results.
Results
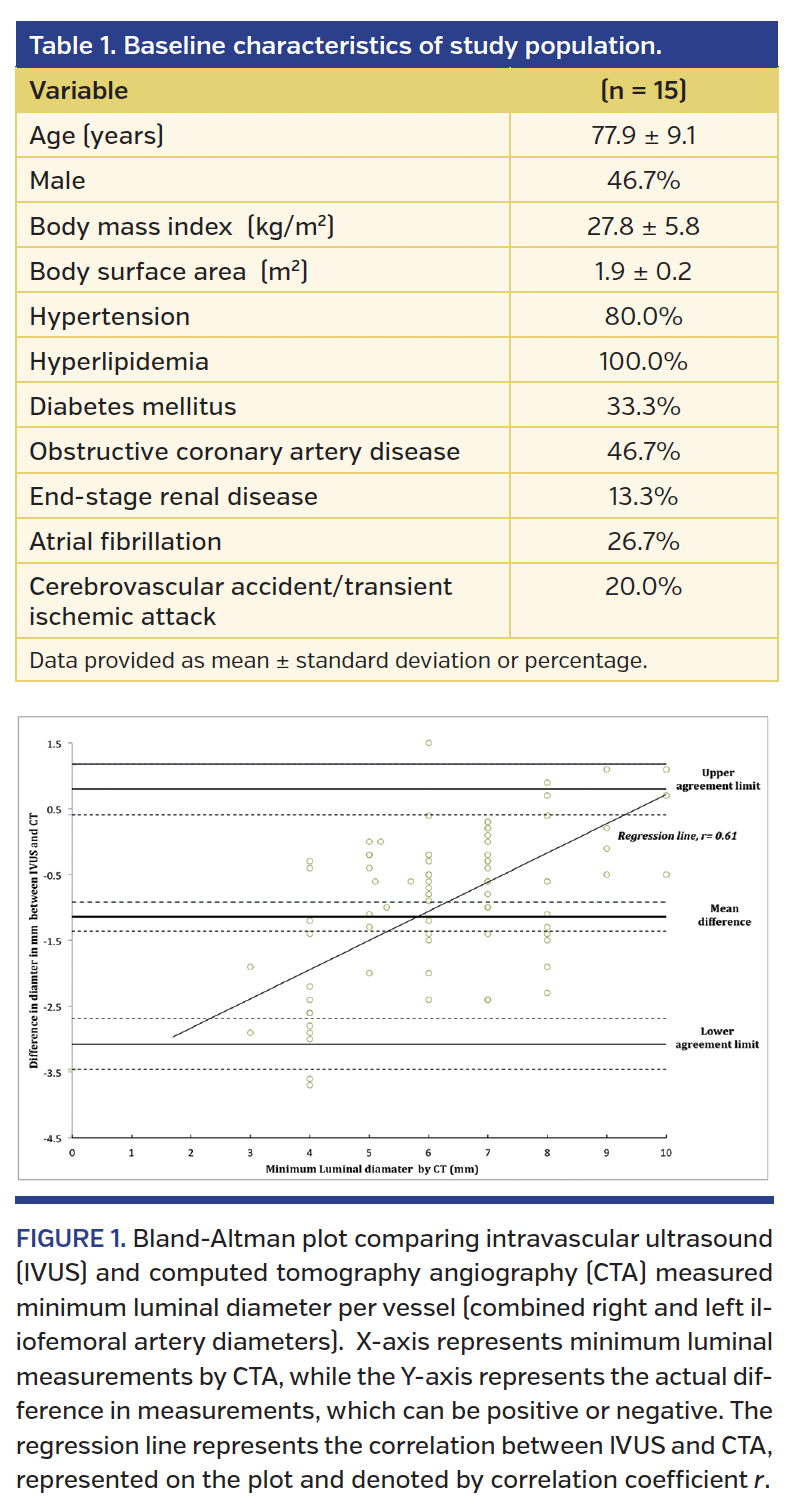
During the study period, a total of 15 TAVR candidates met the inclusion criteria and elected to participate. Mean age was 78 years (range, 52-92 years), 47% were male, and all patients were Caucasian. Cohort characteristics are listed in Table 1.
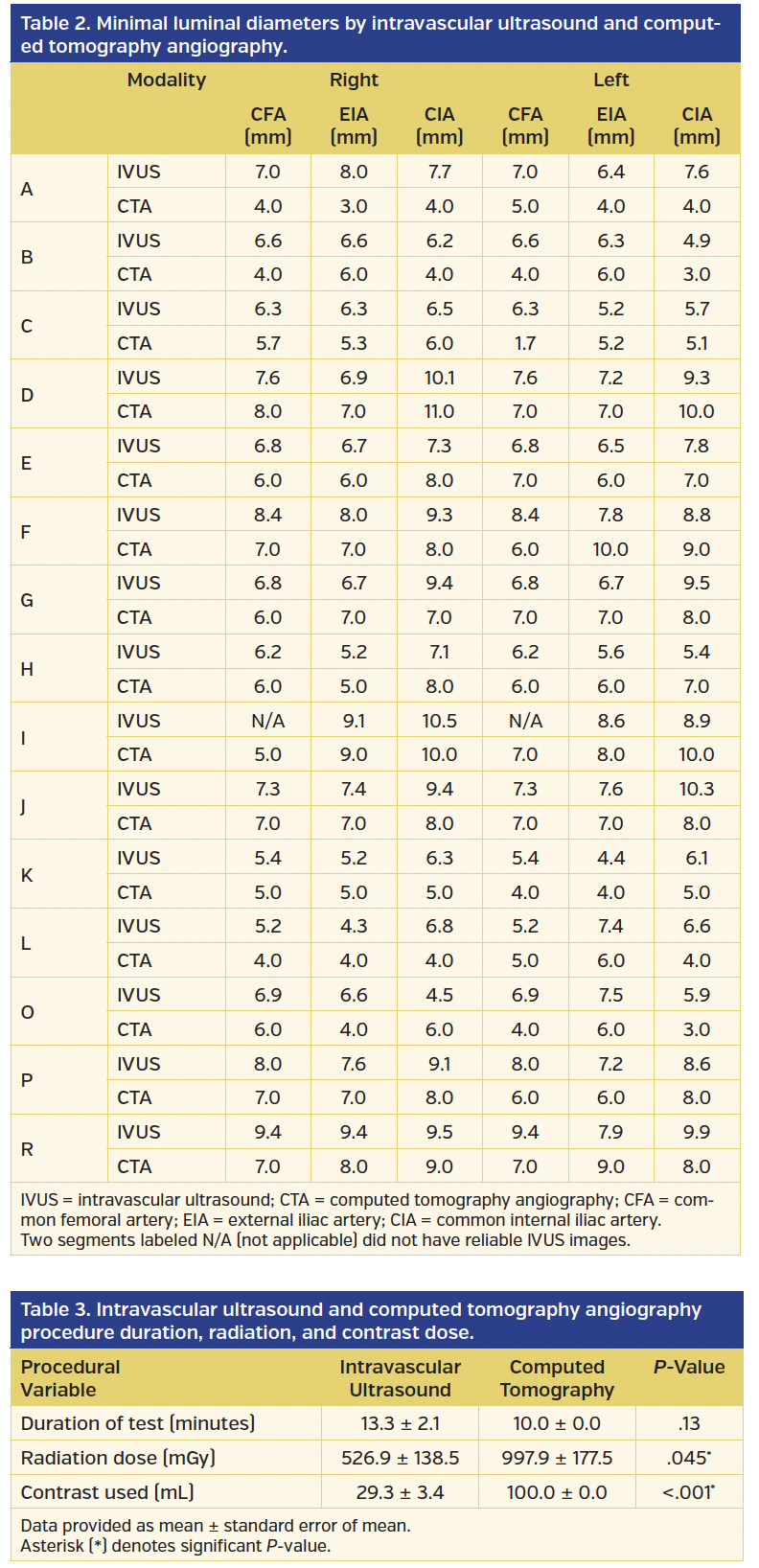
Of the 15 cases, 12 were performed via femoral access, and 3 were performed via radial access. We were able to interrogate all iliac and femoral segments in 14/15 patients. In 1 case, we were unable to visualize the common femoral arteries due to significant tortuosity. No patient experienced a major bleeding-related event, renal injury, or contrast reaction. One patient experienced radial artery injury. The minimum luminal diameter measurements with CTA and IVUS per vessel segment for each patient are represented in Table 2.
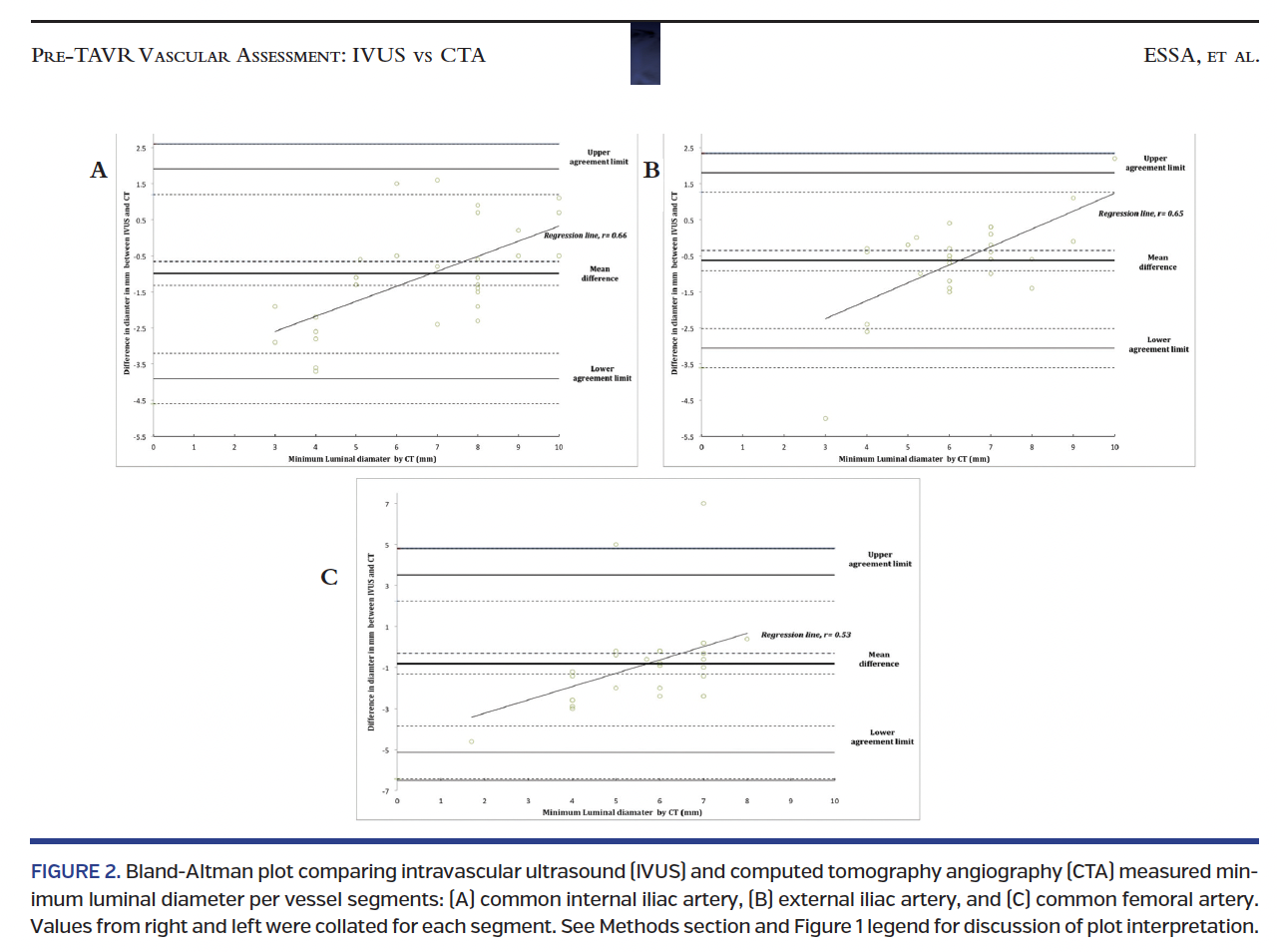
When comparing the per segment minimum luminal diameter, correlation between the two modalities was strong (r=0.6) (Figure 1). Similarly, minimum luminal diameter correlation between CTA and IVUS was strong for common and external iliac arteries when measured per vessel (r=0.65) (Figures 2A, 2B). Correlation was not as strong, but still high, at the level of the common femoral artery (r=0.52) (Figure 2C).
Using Bland-Altman analysis for measures of minimum luminal diameter per segment, bias was significant and IVUS inherently and consistently overestimated the measurements (Figure 1). Similarly, the Bland-Altman plot revealed that bias was significant for measures of minimum luminal diameter per vessel, with IVUS consistently associated with larger diameters than CTA (Figure 2).
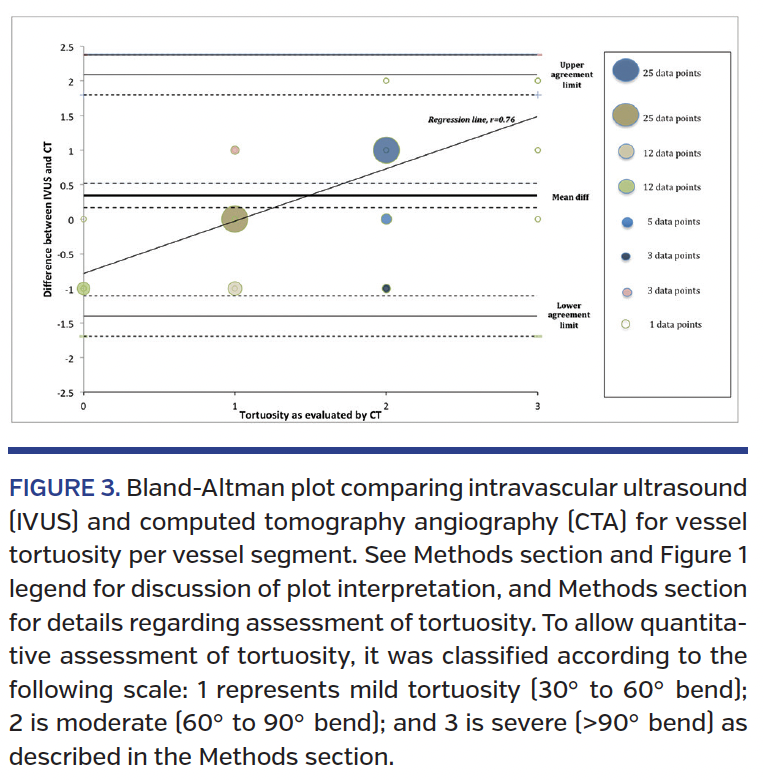
We found that concordance was high between CTA and pre-IVUS iliofemoral angiography for assessment of tortuosity (r=0.75) (Figure 3). Furthermore, we found no evidence of overestimation or underestimation of tortuosity by invasive angiography when compared with the reference CTA (Figure 3).
Analysis also showed that IVUS was associated with lower overall contrast load (29 vs 100 cc; P<.001) and reduced radiation exposure (527 mGy vs 998 mGy; P=.045), but no significant difference in test duration (13.3 minutes vs 10 minutes; P=.12) (Table 3).
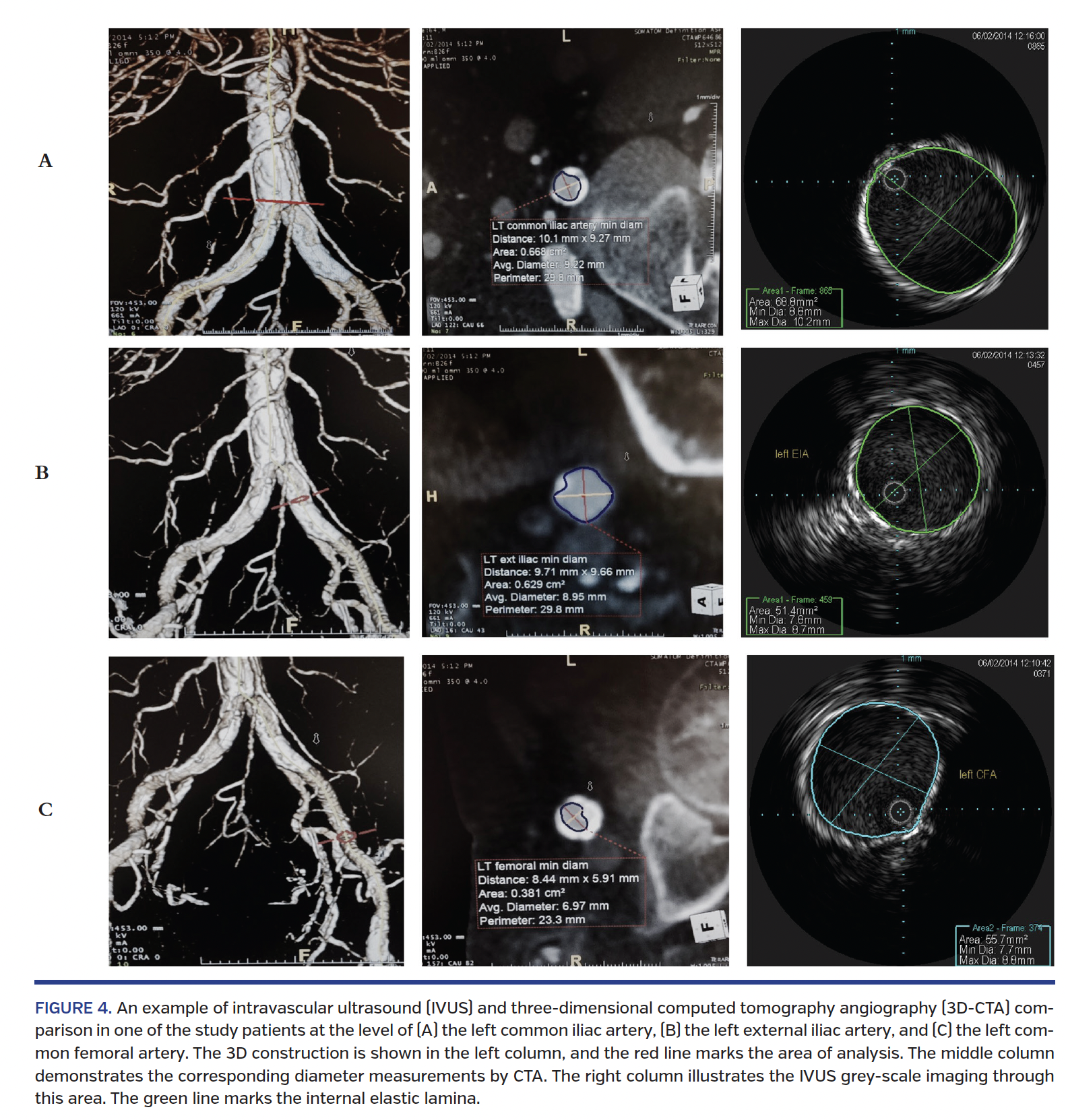
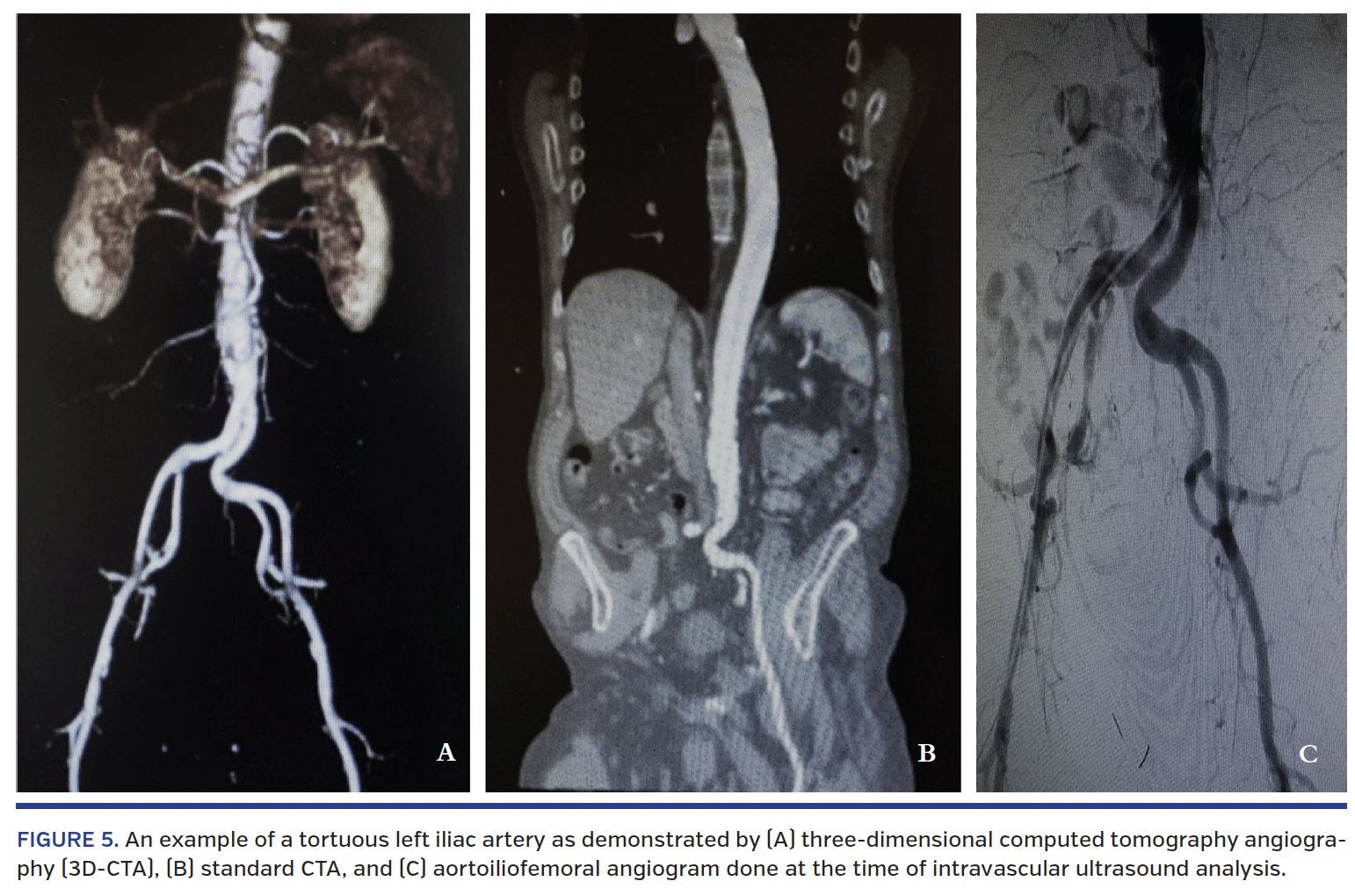
Figure 4 illustrates an example of 3D-CTA and IVUS at different segments in a single vessel. Figure 5 illustrates a severely tortuous left iliac artery as demonstrated by 3D-CTA and pre-IVUS iliofemoral angiogram.
Discussion
CTA is the current standard in pre-TAVR access assessment, although it has limitations related to both accuracy and the use of contrast.15,16 IVUS is a potentially useful alternative or adjunct to CTA for interrogation of iliac and femoral arterial access. Our study revealed the following: (1) there is a strong correlation between CTA and IVUS in the assessment of femoral and iliac artery minimum luminal diameter; (2) IVUS inherently and consistently yields larger diameters when compared with CTA; and (3) IVUS is associated with lower contrast and radiation utilization than CTA.
 To our knowledge, the strong correlation between peripheral arterial IVUS and CTA has not previously been systematically demonstrated. The finding that IVUS-derived diameters were consistently larger than CTA-derived diameters might have significant implications in patients whose arterial diameters are questionably able to accommodate the large sheaths presently utilized for TAVR. A possible explanation for the larger diameter by IVUS is superior spatial resolution. In addition to a more resolved image, IVUS is less prone to artifact resulting from calcium, indwelling stents, or poor vessel opacification compared with CTA. It is also possible that secondary changes in arterial orientation and contour due to access and instrumentation with the IVUS equipment are responsible for some of the differences in measurements. However, vessel
To our knowledge, the strong correlation between peripheral arterial IVUS and CTA has not previously been systematically demonstrated. The finding that IVUS-derived diameters were consistently larger than CTA-derived diameters might have significant implications in patients whose arterial diameters are questionably able to accommodate the large sheaths presently utilized for TAVR. A possible explanation for the larger diameter by IVUS is superior spatial resolution. In addition to a more resolved image, IVUS is less prone to artifact resulting from calcium, indwelling stents, or poor vessel opacification compared with CTA. It is also possible that secondary changes in arterial orientation and contour due to access and instrumentation with the IVUS equipment are responsible for some of the differences in measurements. However, vessel  assessments that occur in tandem with instrumentation might be more informative, as they can approximate the changes that might occur with TAVR valve-delivery systems. This reasoning would require additional evaluation in a larger patient population to be substantiated.
assessments that occur in tandem with instrumentation might be more informative, as they can approximate the changes that might occur with TAVR valve-delivery systems. This reasoning would require additional evaluation in a larger patient population to be substantiated.
Efforts to limit contrast utilization and related risk of contrast nephropathy have been previously studied in the TAVR population. Low-dose CTA scans for assessment of iliofemoral arteries have been described, although with variable overall opacification.17,18 Preliminary 3D magnetic resonance data recently described assessment of the aortoiliofemoral system without administration of contrast medium. The small amount of contrast used in our study was for the iliofemoral angiogram for tortuosity assessment. Whether this is  necessary is a residual question. Tortuosity might be roughly assessed by observing the course of the wire and IVUS catheter by fluoroscopy only, a strategy that warrants additional consideration. However, even if pre-IVUS angiography is completely eliminated, our peripheral IVUS strategy does eliminate the need for contrast, as contrast-enhanced CTA remains the gold-standard modality for establishing appropriate valve sizing. Interestingly, recent preliminary data on a small number of patients suggest accurate IVUS measures when compared with CT in the evaluation of aortic annulus and valve parameters.19 In addition, a number of studies showed non-contrast 3D magnetic resonance angiography to be reliable for the assessment of aortic annulus dimensions and calcifications.20-22
necessary is a residual question. Tortuosity might be roughly assessed by observing the course of the wire and IVUS catheter by fluoroscopy only, a strategy that warrants additional consideration. However, even if pre-IVUS angiography is completely eliminated, our peripheral IVUS strategy does eliminate the need for contrast, as contrast-enhanced CTA remains the gold-standard modality for establishing appropriate valve sizing. Interestingly, recent preliminary data on a small number of patients suggest accurate IVUS measures when compared with CT in the evaluation of aortic annulus and valve parameters.19 In addition, a number of studies showed non-contrast 3D magnetic resonance angiography to be reliable for the assessment of aortic annulus dimensions and calcifications.20-22
IVUS also has the potential to decrease radiation exposure and perhaps reduce cost when performed at the time of the routine pre-TAVR hemodynamic and coronary assessment. Moreover, the data can be interpreted in real time, directly by an operator who is part of the core TAVR team. The potential for increased procedural complications when IVUS is added to coronary angiogram due to longer duration and additional instrumentation is a valid concern. We believe that this additional risk is minimal if IVUS is performed at the time of pre-TAVR coronary angiogram with arterial access already established.
Study limitations. Our study has a number of limitations. First, the study population is relatively small and our findings need to be verified in a larger population. Second, our study did not address iliofemoral arterial calcification. The ability to localize calcification within specific vessel lamina (intima or media) may be relevant in cases where access diameter size is borderline and the presumed distensibility of the vessel is pertinent.9,16 Third, whether an IVUS-only strategy can be predictive of vascular complications at the time of TAVR warrants additional study.
Conclusion
IVUS is a viable alternative to CTA for femoral and iliac arterial assessment prior to TAVR, with comparable accuracy, lower contrast utilization, and less radiation exposure. IVUS is also a valuable adjunct to CTA in patients with borderline femoral access candidacy or CTA artifact.
References
1. Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008;52:e1-e142.
2. Mack MJ, Leon MB, Smith CR, et al: PARTNER 1 trial investigators. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385:2477-2484. Epub 2015 Mar 15.
3. Leon MB, Smith CR, Mack MJ, et al; PARTNER 2 Investigators. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. 2016;374:1609-1620. Epub 2016 Apr 2.
4. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607.
5. Tamburino C, Capodanno D, Ramondo A, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation. 2011;123:299-308.
6. Gurvitch R, Wood DA, Tay EL, et al. Transcatheter aortic valve implantation: durability of clinical and hemodynamic outcomes beyond 3 years in a large patient cohort. Circulation. 2010;122:1319-1327.
7. Eltchaninoff H, Prat A, Gilard M, et al. Transcatheter aortic valve implantation: early results of the FRANCE (FRench Aortic National CoreValve and Edwards) registry. Eur Heart J. 2011;32:191-197.
8. Owen AR, Roditi GH. Peripheral arterial disease: the evolving role of non-invasive imaging. Postgrad Med J. 2011;87:189-198.
9. Toggweiler S, Leipsic J, Binder RK, et al. Management of vascular access in transcatheter aortic valve replacement: part 1: basic anatomy, imaging, sheaths, wires, and access routes. JACC Cardiovasc Interv. 2013;6:643-653.
10. Leber AW, Becker A, Knez A, et al. Accuracy of 64-slice computed tomography to classify and quantify plaque volumes in the proximal coronary system: a comparative study using intravascular ultrasound. J Am Coll Cardiol. 2006;47:672-677.
11. Schepis T, Marwan M, Pflederer T, et al. Quantification of non-calcified coronary atherosclerotic plaques with dual-source computed tomography: comparison with intravascular ultrasound. Heart. 2010;96:610-615.
12. Hayashida K, Lefèvre T, Chevalier B, et al. Transfemoral aortic valve implantation new criteria to predict vascular complications. JACC Cardiovasc Interv. 2011;4:851-858.
13. Giavarina D. Understanding Bland Altman analysis. Biochem Med (Zagreb). 2015;25:141-151.
14. Martin RF. General deming regression for estimating systematic bias and its confidence interval in method-comparison studies. Clin Chem. 2000;46:100-104.
15. Barrett JF, Keat N. Artifacts in CT: recognition and avoidance. Radiographics. 2004;24:1679-1691.
16. Toggweiler S, Leipsic J, Binder RK, et al. Management of vascular access in transcatheter aortic valve replacement: part 2: vascular complications. JACC Cardiovasc Interv. 2013;6:767-776.
17. Joshi SB, Mendoza DD, Steinberg DH, et al. Ultra-low-dose intra-arterial contrast injection for iliofemoral computed tomographic angiography. JACC Cardiovasc Imaging. 2009;2:1404-1411.
18. Nietlispach F, Leipsic J, Al-Bugami S, Masson JB, Carere RG, Webb JG. CT of the ilio-femoral arteries using direct aortic contrast injection: proof of feasibility in patients screened towards percutaneous aortic valve replacement. Swiss Med Wkly. 2009;139:458-462.
19. de Cillis E, Dachille A, Giardinelli F, Acquaviva T, Bortone AS. Accuracy of intravascular ultrasound evaluation for the assessment of native valve measures in patients undergoing TAVI: preliminary results. Surg Technol Int. 2016 Jul 29 (Epub ahead of print).
20. Ruile P, Blanke P, Krauss T, et al. Pre-procedural assessment of aortic annulus dimensions for transcatheter aortic valve replacement: comparison of a non-contrast 3D MRA protocol with contrast-enhanced cardiac dual-source CT angiography. Eur Heart J Cardiovasc Imaging. 2016;17:458-466. Epub 2015 Jul 27.
21. Renker M, Varga-Szemes A, Schoepf UJ, et al. A non-contrast self-navigated 3-dimensional MR technique for aortic root and vascular access route assessment in the context of transcatheter aortic valve replacement: proof of concept. Eur J Radiol. 2016;26:951-958. Epub 2015 Jul 20.
22. Gopal A, Grayburn PA, Mack M, et al. Non-contrast 3D CMR imaging for aortic valve annulus sizing in TAVR. JACC Cardiovasc Imaging. 2015;8:375-378.
From the 1Department of Cardiovascular Medicine, Mount Carmel Healthcare System, Columbus, Ohio; 2Department of Cardiovascular Medicine, The Ohio State Wexner Medical Center, Columbus, Ohio; and 3Summa Health System, Akron, Ohio.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Bittenbender is a proctor/consultant for Edwards Lifesciences. The remaining authors report no conflicts of interest regarding the content herein.
Manuscript submitted August 9, 2016 and accepted August 15, 2016.
Address for correspondence: Scott Lilly, MD, 410 W. 10th Ave, 1 Maloney Building, Columbus, OH 43210. Email: Scott.Lilly@osumc.edu













