

Conservative Management of Pneumopericardium: A Case of Unexpected Success
J INVASIVE CARDIOL 2023;37(9):E75-E83
Key words: pneumopericardium, computed tomography, pericardiocentesis
A 79-year-old male with severe aortic stenosis was admitted with syncope and cranioencephalic traumatism with major nasal hemorrhage. While being prepared for surgical aortic valve replacement, a high-degree atrioventricular block was detected and a definite pacemaker was implanted. Throughout the preoperative workup, incidental findings of pulmonary thromboembolism were noted and low dose subcutaneous enoxaparin 40 mg id was started, bearing in mind frailty status and the previous hemorrhage. A few days later, the patient presented with gastrointestinal bleeding and consequent hemorrhagic shock.
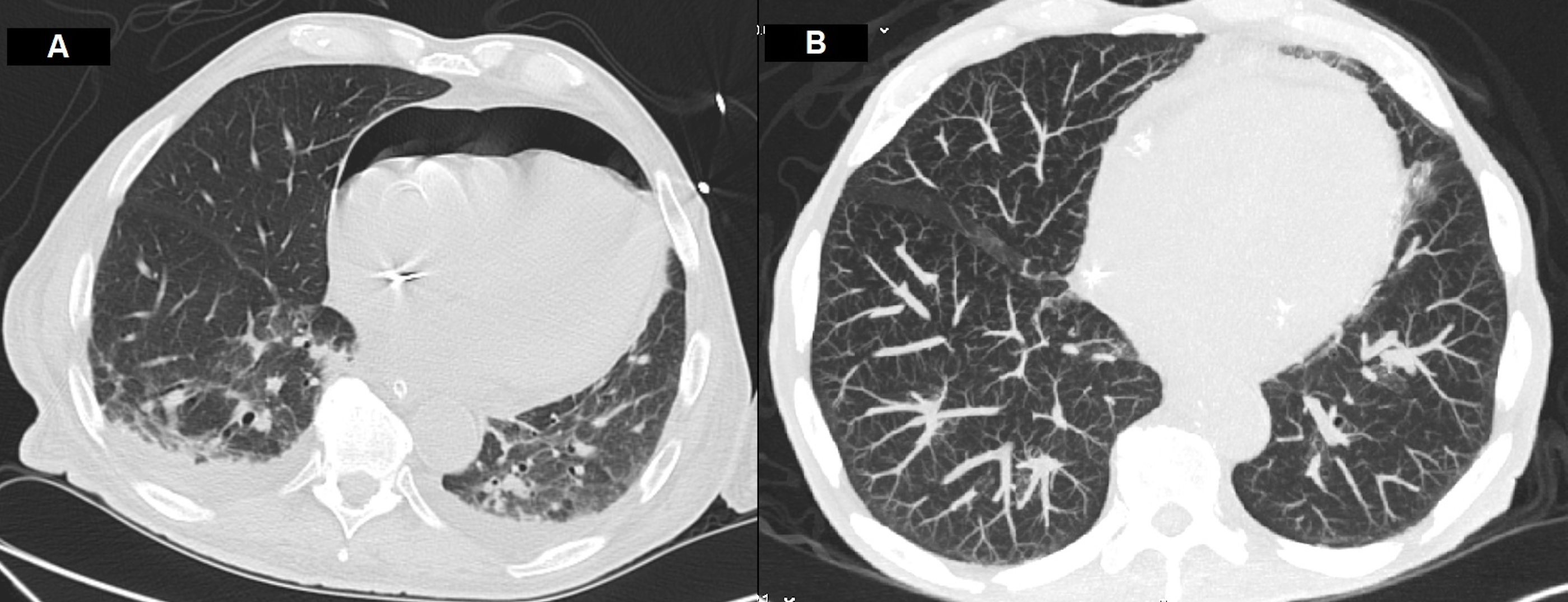
Targeted treatment with fluid challenge, blood transfusion, proton pump inhibitor perfusion, and aminergic support was initiated. While preparing for endoscopy, shock worsened, with arterial systolic pressure dropping to 30-40 mmHg. The echocardiographic evaluation showed a new moderate pericardial effusion. Emergent pericardiocentesis was performed, draining 250 ml of serohematic fluid, which led to clinical improvement. Upper gastrointestinal endoscopy showed abundant clots and active bleeding. Angio-CT scan, aiming at identifying the bleeding vessel for embolization, unexpectedly showed pneumopericardium related to the pericardial drain (Figure 1A), a small pneumothorax, and a moderate pneumoperitoneum. The pericardial drain was removed and conservative treatment was adopted, considering the extremely high operative risk. Good response to treatment ultimately made it possible to discharge the patient home 15 days later, under optimized medical therapy. Subsequently, a month later, he was admitted with symptomatic heart failure and syncopal events. At this point, the possibility of transcatheter aortic valve implantation was considered and the patient was re-evaluated with a CT scan, which showed complete reabsorption of the pneumopericardium (Figure 1B).
Affiliations and Disclosures
From 1Department of Cardiology, Centro Hospitalar e Universitário de Coimbra, Coimbra, Portugal, 2Faculdade de Medicina da Universidade de Coimbra, Coimbra, Portugal.
Disclosure: The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted January 27, 2023.
Address for correspondence: Ana Rita M. Gomes, MD, MSc, Centro Hospitalar e Universitário de Coimbra, Quinta dos Vales, 3041-801, Coimbra, Portugal, Email: gomes.anarm@gmail.com











