

Retrieval of a Severely Double-Kinked Catheter in the Right Brachial Artery by Internal Fixation With a Peripheral Angioplasty Balloon
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 55-year-old female patient with unstable angina and accelerated hypertension was planned for invasive coronary and renal angiogram. A 6-French (Fr) radial sheath (Terumo) was introduced, and coronary angiogram done with a 5-Fr Tiger catheter (Terumo) revealed insignificant disease. Renal angiogram was performed with a 5-Fr 125-cm Judkins Right (JR) catheter (Medtronic). Significant difficulty was encountered while doing renal angiogram due to the aortic tortuosity.
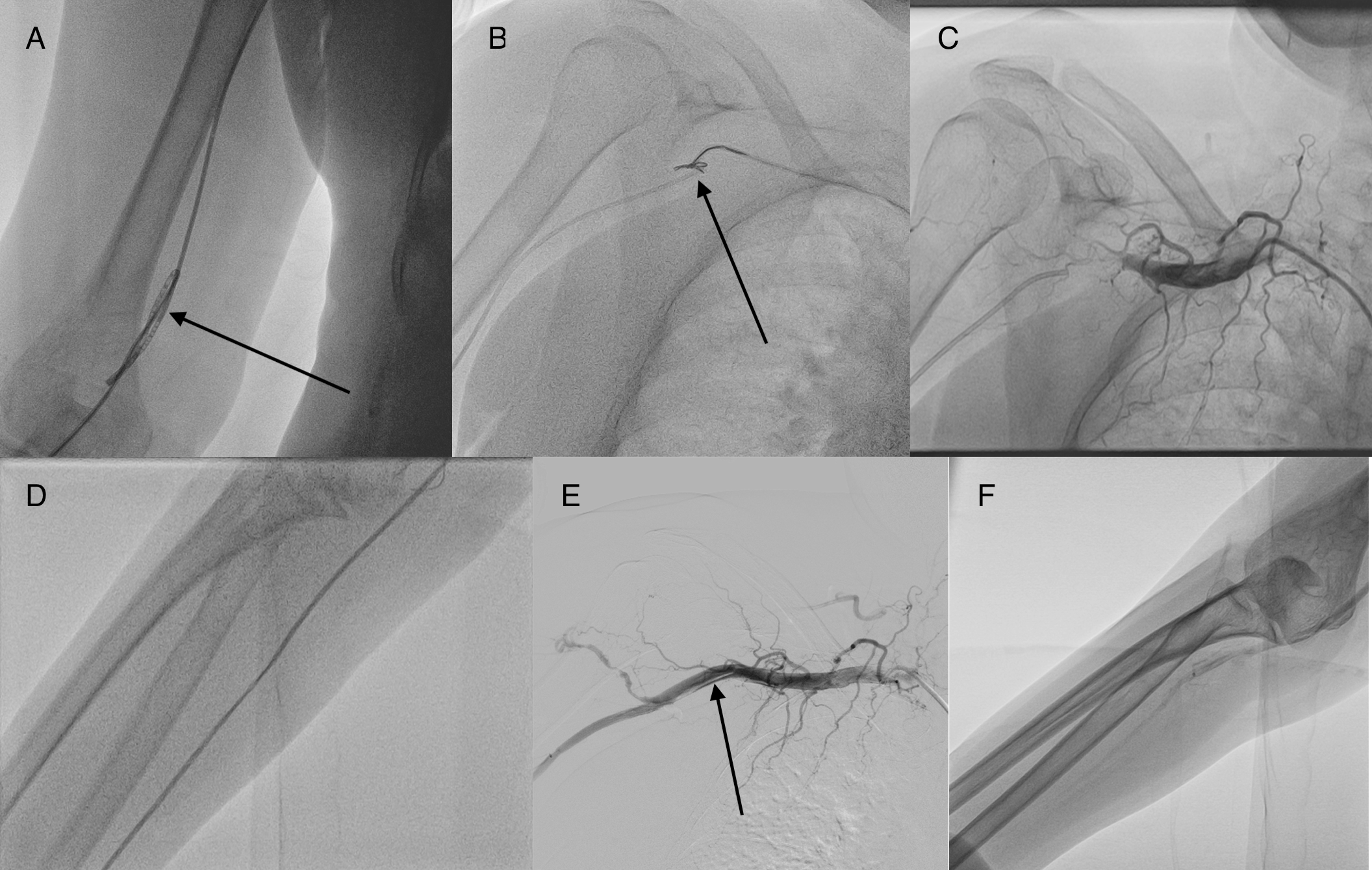
After the renal angiogram, there was a loss of arterial pressure tracing. Fluoroscopy revealed kinking and double knotting of the catheter at the level of elbow (Figure, A; Video 1) with severe spasm. All previously described techniques to open the loop, including rotating the catheter in the opposite direction, use of 0.035-inch guidewire and coronary 0.014-inch guidewire to cross the kink, and mother-and-child technique, failed. Use of a sphygmomanometer inflated above the kink to supra-systemic pressure also failed. Multiple attempts lasting a total of 120 minutes to snare the tip of the kinked catheter with a 6-Fr gooseneck snare (Lifetech) (Figure, B; Video 2) in a 6-Fr JR catheter from 7-Fr right femoral access failed due to aortic tortuosity allowing limited movement of the snare and severe radial spasm allowing minimal movement of the kinked catheter.
At this time, we contemplated subjecting the patient to surgical removal. A diagnostic angiogram showed thrombotic occlusion of the axillary artery (Figure, C; Video 3) due to repeated attempts to snare, despite activated clotting time being greater than 250 seconds. A glidewire (Terumo) was advanced across the occlusion and a peripheral 5 × 100-mm Ultraverse balloon (Becton Dickinson) was inflated for the vascular thrombosis. The inflated balloon fixed the catheter tip internally, and gentle pulling of the kinked catheter opened the loop (Figure, D; Video 4). Subsequently, a 0.035-inch guidewire (Terumo) was introduced and the kinked catheter was removed (Video 5). An angiogram showed axillary artery dissection (Figure, E; Video 6) with acceptable distal flow (Figure, F; Video 7), which was managed conservatively. The total procedure time was 240 minutes. Low molecular weight heparin was given for 48 hours, and the patient remained asymptomatic at discharge with no signs of limb ischemia.
Affiliations and Disclosures
From the Department of Cardiology, U.N. Mehta Institute of Cardiology and Research Centre, Ahmedabad, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Kewal Kanabar, MD (AIIMS, New Delhi), DM (PGIMER, Chandigarh), Associate Professor, Department of Cardiology, U.N. Mehta Institute of Cardiology and Research Centre, Ahmedabad-380016, India. Email: kewal.kanabar14@gmail.com; X: @KewalKanabar












