

Endovascular Repair of Iatrogenic Inferior Vena Cava Stenosis in a Live Kidney Donor
Abstract
We report the endovascular treatment of a rare complication of iatrogenic inferior vena cava stenosis following a right live donor nephrectomy. This report highlights the clinical presentation, imaging, and management of such a case.
VASCULAR DISEASE MANAGEMENT 2012:9(11):E198-E200
Key words: angioplasty, balloon angioplasty, inferior vena cava, interventional radiology
_____________________________________
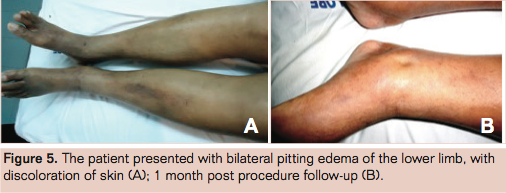
A 58-year-old male live related donor with no comorbid factors and normal renal vasculature on preoperative CT angiography was planned for a right nephrectomy. The right kidney was chosen as the left had a better relative function on isotope scan and also the right kidney had a relatively short renal vein, which would allow little room for cross clamp and anastomosis. Laparoscopic nephrectomy was not possible as there were dense adhesions, and an uneventful open donor nephrectomy was carried out by extraperineal approach. One month postoperatively he presented with progressive swelling of both legs.
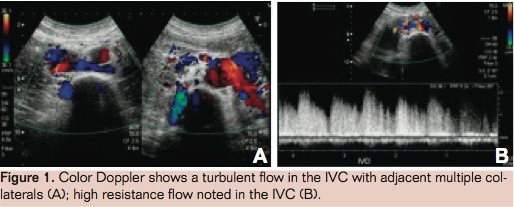
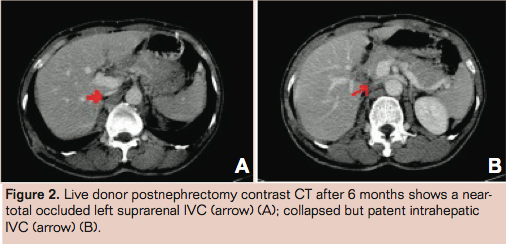
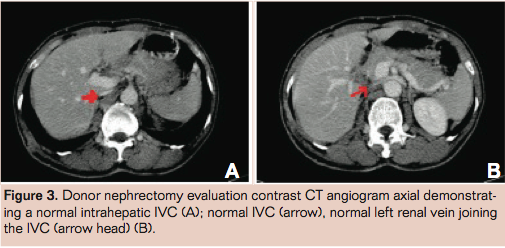
On examination the patient had typical features of inferior vena cave (IVC) syndrome with pitting edema and abdominal wall veins. A Doppler study showed a dilated IVC with a nonvisualized infrahepatic segment above the renal vein drainage and adjacent multiple collaterals (Figure 1). There was severe segmental narrowing of the suprarenal–infrahepatic segment of IVC on contrast enhanced computed tomography (CT) scan (Figure 2). The CT done prior to nephrectomy had shown a patent IVC (Figure 3).
A venogram was performed under local anesthesia through a right transfemoral approach, which demonstrated a near total occlusion of the cranial IVC to the left renal vein with opacification of multiple paraspinal veins (Figure 4). The stenosis was crossed with a 0.035” hydrophilic wire (Terumo) and a 5F Van Schie seeking catheter (Cook). Balloon angioplasty was performed using 8mm, 10mm, and 12mm balloons (Cook) serially. There was good restoration of the lumen.
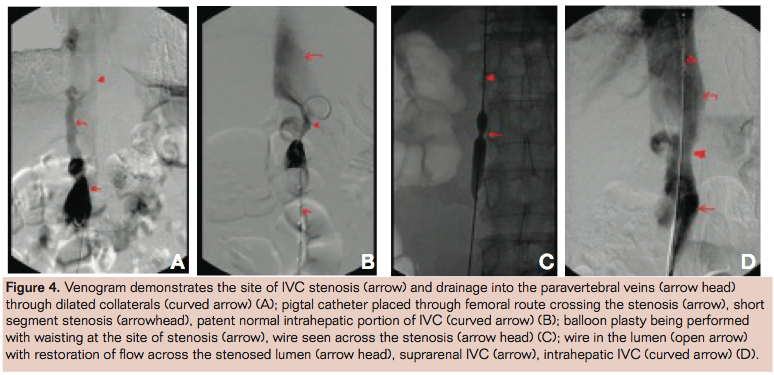
The pressure gradient across the stenosis was 49 mm Hg before angioplasty, which reduced to 24 mm Hg after the procedure. The patient showed signs of improvement. At 1 month, follow-up showed significant improvement of the lower limbs.
Discussion
Obstruction of the IVC can be congenital or acquired. The fully developed IVC is a complex structure derived from different segments of multiple paired longitudinal embryonic veins and the interconnections between them.1,2 The complex development of IVC can cause webbing and strictures near the liver and diaphragm. Obstruction to the normal channel may result in the efficient collateral function like drainage through azygous and semi-azygous veins. Patients who have obstructed IVC may present with debilitating lower limb pain and swelling, back pain, weakness, and venous stasis ulceration.3
Acquired obstructions of the IVC are equally common and can result from dehydration, sepsis, pelvic inflammatory disease, coagulopathy, congestive heart failure, trauma, immobility, severe exertion, or iatrogenic causes (eg, placement of an IVC filter or surgery). Less commonly they are caused by tumor invasion, extrinsic compression, and intrinsic caval disease.2 During a right donor nephrectomy, a 1 mm to 2 mm cuff of IVC routinely is taken to facilitate anastomosis without any compromise to the lumen of the IVC. In our case we assume that it is a tight vascular stricture, since no scar tissue was visible on the CT scan.
IVC occlusion at various levels can be managed either surgically or endovascularly. Surgical reconstructions of venous occlusive disease are rarely performed and the long-term patency, clinical outcome, and risk factors for graft occlusion are less understood.4 However, an endoluminal approach is often effective in relieving symptoms in patients and should be considered as a first-line treatment.3 Endoluminal treatment can be performed with either balloon angioplasty or stenting. Results of balloon angioplasty can be disappointing in cases of chronic obstruction and in recoil lesions. Relevant information regarding long-term restenosis rate of the IVC after angioplasty cannot be found in the literature.
In the case of this patient we knew that he had an acquired postsurgical stenosis, on the basis of the preoperative CT scan. We restored the flow and normalized the pressures using graded angioplasty. A backup stent was planned, although it was not necessary.
Conclusion
Postpoerative IVC stenosis or occlusion is a rare iatrogenic complication reported in live donor nephrectomy.5 Endovascular treatment in such situations is safe and effective.
References
- Kapur S, Paik E, Rezaei A, Vu DN. Where there is blood, there is a way: unusual collateral vessels in superior and inferior vena cava obstruction. Radiographics. 2010;30(1):67-78.
- Raju S, Hollis K, Neglen P. Obstructive lesions of the inferior vena cava: Clinical features and endovenous treatment. J Vasc Surg. 2006;44(4):820-827.
- Razavi MK, Hansch EC, Kee ST, Sze DY, Semba CP, Dake MD. Chronically occluded inferior vena cavae: endovascular treatment. Radiology. 2000;214(1):133-138.
- Jost CJ, Gloviczki P, Cherry KJ Jr, et al. Surgical reconstruction of iliofemoral veins and the inferior vena cava for nonmalignant occlusive disease. J Vasc Surg. 2001;33(2):320-328.
- Su LM, Ratner LE, Montgomery RA, et al. Laparoscopic live donor nephrectomy trends in donor and recipient morbidity following 381 consecutive cases. Ann Surg. 2004;240(2):358-363.
______________________________
Editor’s Note: Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript received April 27, 2012, provisional acceptance given May 20, 2012, final version accepted May 21, 2012.
Address for correspondence: Suraj Mammen, MBBS, MD, Department of Radiology, Christian Medical College, Vellore, Tamil Nadu, India. Email: surajmammen77@gmail.com
